

Medication adherence issues in patients treated for COPD
- PMID: 18990964
- PMCID: PMC2629978
- DOI: 10.2147/copd.s3036
Medication adherence issues in patients treated for COPD
Abstract
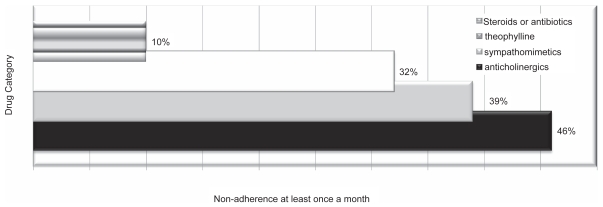
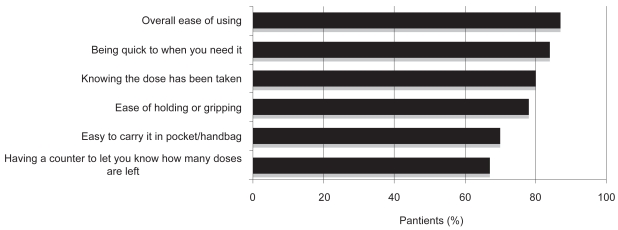
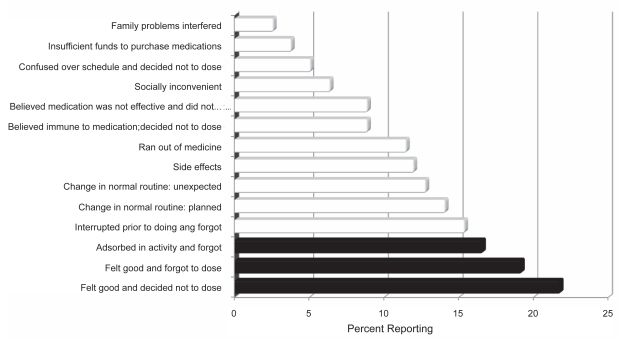
Although medical treatment of COPD has advanced, nonadherence to medication regimens poses a significant barrier to optimal management. Underuse, overuse, and improper use continue to be the most common causes of poor adherence to therapy. An average of 40%-60% of patients with COPD adheres to the prescribed regimen and only 1 out of 10 patients with a metered dose inhaler performs all essential steps correctly. Adherence to therapy is multifactorial and involves both the patient and the primary care provider. The effect of patient instruction on inhaler adherence and rescue medication utilization in patients with COPD does not seem to parallel the good results reported in patients with asthma. While use of a combined inhaler may facilitate adherence to medications and improve efficacy, pharmacoeconomic factors may influence patient's selection of both the device and the regimen. Patient's health beliefs, experiences, and behaviors play a significant role in adherence to pharmacological therapy. This manuscript reviews important aspects associated with medication adherence in patients with COPD and identifies some predictors of poor adherence.
Figures
References
-
- Aaron SD, Vandemheen KL, Fergusson D, et al. Canadian Thoracic Society/Canadian Respiratory Clinical Research Consortium. Tiotropium in Combination with Placebo, Salmeterol, or Fluticasone – Salmeterol for Treatment of Chronic Obstructive Pulmonary Disease. Ann Intern Med. 2007;146:545–55. - PubMed
-
- Andersson K, Melander A, Svensson C, et al. Repeat prescriptions: refill adherence in relation to patient and prescriber characteristics, reimbursement level and type of medication. Eur J Public Health. 2005;15:621–6. - PubMed
-
- Balzano G, Battiloro R, Biraghi M, et al. Effectiveness and acceptability of a domiciliary multidrug inhalation treatment in elderly patients with chronic airflow obstruction: metered dose inhaler versus jet nebulizer. J Aerosol Med. 2000;13:25–33. - PubMed
-
- Barry MJ. Chronic obstructive pulmonary disease: developing comprehensive management. Respir Care. 2003;48:1225–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
