

Systemic impairment in relation to disease burden in patients with moderate COPD eligible for a lifestyle program. Findings from the INTERCOM trial
- PMID: 18990973
- PMCID: PMC2629991
- DOI: 10.2147/copd.s2588
Systemic impairment in relation to disease burden in patients with moderate COPD eligible for a lifestyle program. Findings from the INTERCOM trial
Abstract
Introduction: In contrast with the frequency distribution of chronic obstructive pulmonary disease (COPD) stages in the population, in which the majority of the patients is classified as GOLD 2, much less information is available on the prevalence and implications of systemic manifestations in less severe patients relative to GOLD 3 and 4.
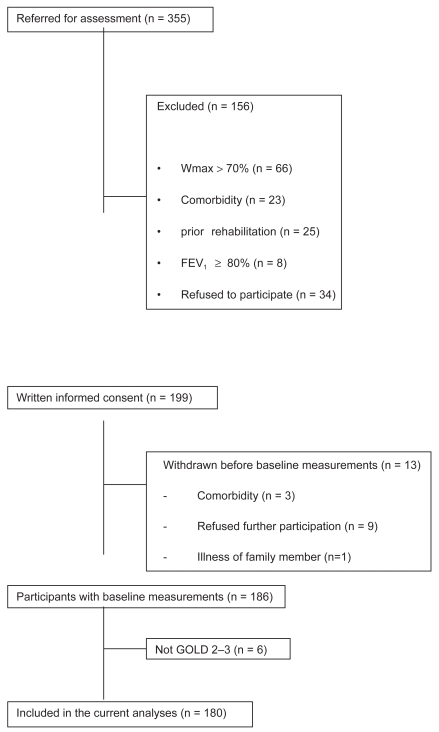
Aim: To characterize local and systemic impairment in relation to disease burden in a group of GOLD 2 COPD patients (n = 127, forced expiratory volume in one second (SD): 67 (11)% pred) that were eligible for the Interdisciplinary Community-based COPD management (INTERCOM) trial.
Methods: Patients were included for this lifestyle program based on a peak exercise capacity (Wmax) < 70% of predicted. Metabolic and ventilatory response to incremental cycle ergometry, 6 minute walking distance (6MWD), constant work rate test (CWR), lung function, maximal inspiratory pressure (Pimax), quadriceps force (QF), quadriceps average power (QP) (isokinetic dynamometry), handgrip force (HGF) and body composition were measured. Quality of life (QoL) was assessed by the St. George's Respiratory Questionnaire (SGRQ) and dyspnea by the modified Medical Research Council (MRC) dyspnea scale. Exacerbations and COPD-associated hospital admissions in 12 months prior to the start of the study were recorded. Burden of disease was defined in terms of exercise capacity, QoL, hospitalization, and exacerbation frequency. GOLD 2 patients were compared with reference values and with GOLD 3 patients who were also included in the trial.
Results: HGF (77.7 (18.8) % pred) and Pimax (67.1 (22.5)% pred) were impaired in GOLD 2, while QF (93.5 (22.5)% pred) was only modestly decreased. Depletion of FFM was present in 15% of weight stable GOLD 2 patients while only 2% had experienced recent involuntary weight loss. In contrast to Wmax, submaximal exercise capacity, muscle function, and body composition were not significantly different between GOLD 2 and 3 subgroups. Body mass index and fat-free mass index were significantly lower in smokers compared to ex-smokers. In multivariate analysis, QF and diffusing capacity (DLco) were independently associated with Wmax and 6 MWD in GOLD 2 while only 6 MWD was identified as an independent determinant of health-related QoL. HGF was an independent predictor of hospitalization.
Conclusions: This study shows that also in patients with moderate COPD, eligible for a lifestyle program based on a decreased exercise capacity, systemic impairment is an important determinant of disease burden and that smoking affects body composition.
References
-
- Baarends EM, Schols AM, Mostert R, et al. Peak exercise response in relation to tissue depletion in patients with chronic obstructive pulmonary disease. Eur Respir J. 1997;10:1856–61. - PubMed
-
- Black LF, Hyatt RE. Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Respir Dis. 1969;99:696–702. - PubMed
-
- Bourbeau J, Julien M, Maltais F, et al. Reduction in hospital utilization in patients with chronic obstructive pulmonary disease. Arch Intern Med. 2003;163:585–91. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
