

Implementation of intermittent preventive treatment in pregnancy with sulphadoxine/pyrimethamine (IPTp-SP) at a district health centre in rural Senegal
- PMID: 18992140
- PMCID: PMC2588629
- DOI: 10.1186/1475-2875-7-234
Implementation of intermittent preventive treatment in pregnancy with sulphadoxine/pyrimethamine (IPTp-SP) at a district health centre in rural Senegal
Abstract
Background: Intermittent preventive treatment with sulphadoxine-pyrimethamine (SP) is recommended for reducing the risk of malaria in pregnancy and its consequences on mothers and babies (IPTp-SP). Indicators of implementation and effects of IPTp-SP were collected in a rural clinic in Southern Senegal.
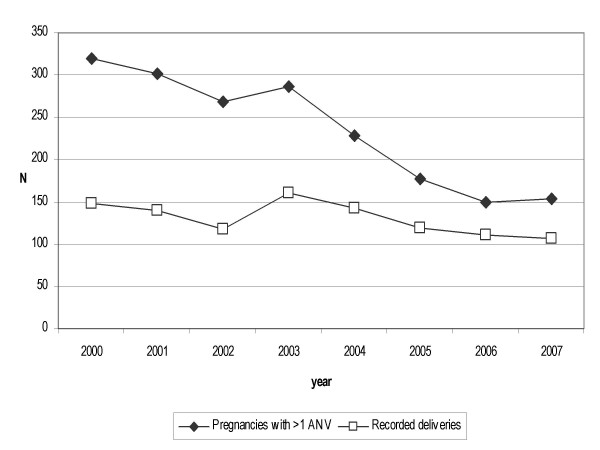
Methods: Women seen routinely at the antenatal clinic (ANC) of a rural dispensary during 2000-2007. Deployment of IPTp-SP started in January 2004. Inspection of antenatal and outpatient clinic registries of the corresponding period.
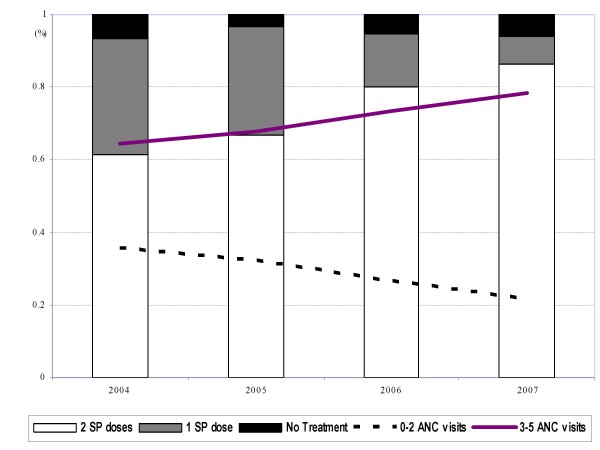
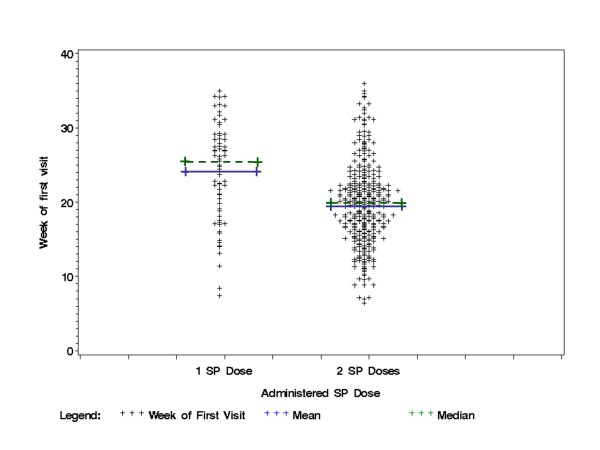
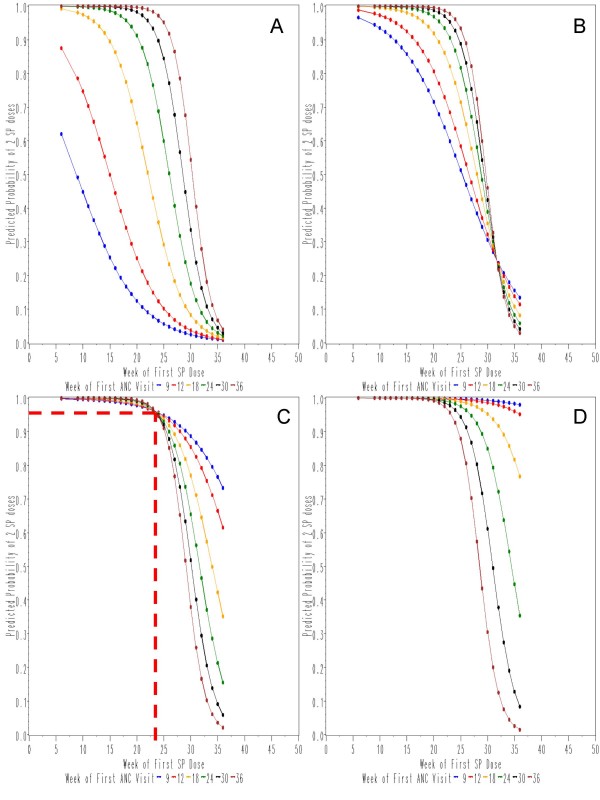
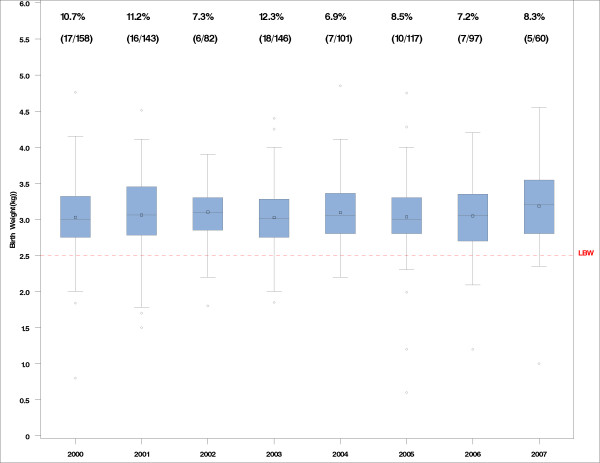
Results: Between 1st January 2000 and 30th April 2007, 1,781 women of all gravitidities and parities attended the ANC with 965 deliveries (606 and 398 respectively since 1st January 2004, when IPTp-SP was started.) 69% of women were seen > or = 3 times; 95% received at least one dose and 70% two doses of SP (from 61% in 2004 to 86% in 2007). The first visit, first and second dose of SP occurred at a median week 20, 22 and 31. The probability of receiving two doses was > 80% with > or = 3 antenatal visits and a first dose of SP by week 20.The prevalence of maternal malaria was low and similar pre- (0.7%) and during IPTp (0.8%). Effects on of low birth weight (LBW, < 2.5 kg) were non-statistically significant. The prevalence of LBW was 10.8% pre- and 7.7% during IPTp deployment (29% risk reduction, p = 0.12).Unfavourable pregnancy outcomes numbered 72 (7.5% of pregnancies with known outcome), including 30 abortions and 42 later deaths (late foetal deaths, stillbirth, peri-natal) of which 13 with one or more malformations (1.35% of all recorded deliveries).
Conclusion: The implementation of IPTp-SP was high. Early attendance to ANC favours completion of IPTp-SP. The record keeping system in place is amenable to data extraction and linkage. A model was developed that predicts optimal compliance to two SP doses, and could be tested in other settings. Maternal malaria was infrequent and unaffected by IPTp-SP. The risk of LBW was lower during IPT implementation but the difference was non-significant and could have other explanations.
Figures
References
-
- World Health Organization . Malaria in pregnancy Guidelines for measuring key monitoring and evaluation indicators. WHO; 2007.
-
- Garner P, Gülmezoglu AM. Drugs for preventing malaria in pregnant women. Cochrane Database Syst Rev. 2006;4:CD000169. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
