

Transperineal three-dimensional ultrasound imaging for detection of anatomic defects in the anal sphincter complex muscles
- PMID: 18996750
- PMCID: PMC2835972
- DOI: 10.1016/j.cgh.2008.08.019
Transperineal three-dimensional ultrasound imaging for detection of anatomic defects in the anal sphincter complex muscles
Abstract
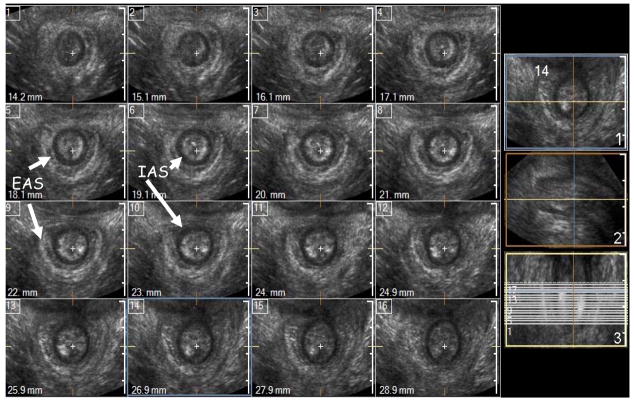
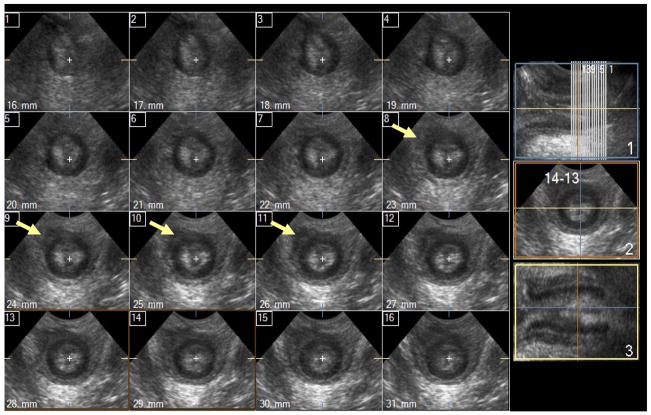
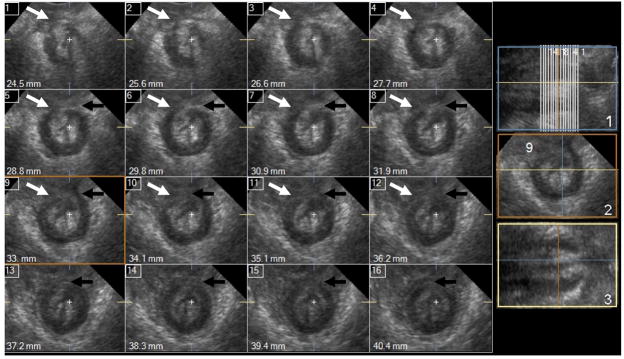
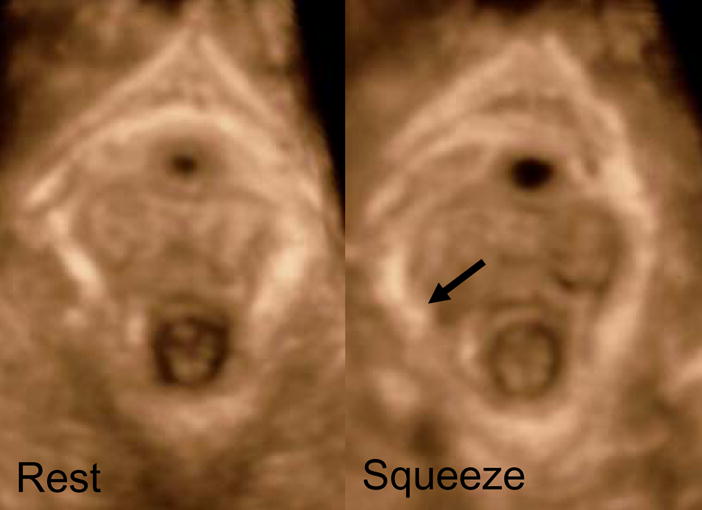
Background & aims: Three-dimensional ultrasound (3D-US) imaging is a powerful tool to visualize various components of the anal sphincter complex, that is, the internal anal sphincter (IAS), the external anal sphincter (EAS), and the puborectalis muscle (PRM). Our goal was to determine the reliability of the 3D-US imaging technique in detecting morphologic defects in the IAS, EAS, and PRM.
Methods: Transperineal 3D-US images were obtained in 3 groups of women: nulliparous (n = 13), asymptomatic parous (n = 20), and patients with fecal incontinence (FI) (n = 25). The IAS and EAS were assessed to determine the craniocaudal length of defects and were scored as follows: 0 = normal, 1 = less than 25%, 2 = 25% to 50%, 3 = 50% to 75%, and 4 = greater than 75%. The 2 PRM hemislings were scored separately as follows: 0 = normal, 1 = less than 50% abnormal, and 2 = greater than 50% length abnormal. Subjects were grouped according to the score as follows: normal (score 0), minor abnormality (scores of 1 and 2), and major abnormality (scores of 3 and 4). Three observers performed the scoring.
Results: The 3D-US allowed detailed evaluation of the IAS, EAS, and PRM. The inter-rater reliability for detecting the defects ranged between 0.80 and 0.95. Nullipara women did not show any significant defect but the defects were quite common in asymptomatic parous and FI patients. The prevalence of defects was greater in the FI patients as compared with the asymptomatic parous women.
Conclusions: 3D-US yields reliable assessment of morphologic defects in the anal sphincter complex muscles.
Conflict of interest statement
Figures

References
-
- Sultan AH, Kamm MA, Hudson CN, Thomas JM, Bartram CI. Anal-sphincter disruption during vaginal delivery. N Engl J Med. 1993;329(26):1905–11. - PubMed
-
- Fernandez-Fraga X, Azpiroz F, Malagelada JR. Significance of pelvic floor muscles in anal incontinence. Gastroenterology. 2002;123(5):1441–50. - PubMed
-
- Bharucha AE. Fecal incontinence. Gastroenterology. 2003;124(6):1672–85. - PubMed
-
- DeLancey JO. The anatomy of the pelvic floor. Curr Opin Obstet Gynecol. 1994;6(4):313–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
