

Acute graft-versus-host disease after unrelated donor umbilical cord blood transplantation: analysis of risk factors
- PMID: 18997171
- PMCID: PMC2656268
- DOI: 10.1182/blood-2008-07-163238
Acute graft-versus-host disease after unrelated donor umbilical cord blood transplantation: analysis of risk factors
Abstract
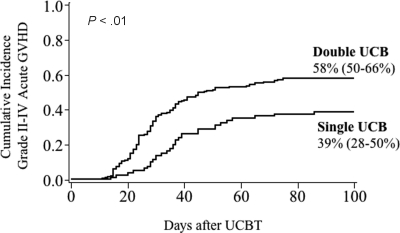
Acute graft-versus-host disease (GVHD) occurs less frequently after umbilical cord blood transplantation (UCBT). More recent investigations include the use of 2 partially human leukocyte antigen (HLA)-matched UCB units, or double UCB graft, to meet the minimum cell-dose requirement. The purpose of this analysis was to assess the relative risk of acute GVHD in 265 consecutive patients receiving transplants with UCB graft composed of 1 (n = 80) or 2 (n = 185) units. The incidence of grade III-IV acute GVHD was similar between cohorts. However, the incidence of grade II-IV acute GVHD was higher among double UCBT recipients (58 vs 39%, P < .01). Three risk factors for grade II-IV acute GVHD were identified in multiple regression analysis: use of 2 UCB units, use of nonmyeloablative conditioning, and absence of antithymocyte globulin in the conditioning regimen. Transplantation-related mortality (TRM) at 1 year, however, was significantly lower after double UCBT (24 vs 39%, P = .02) even if recipients had grade II-IV acute GVHD (20 vs 39%, P = .05). These data suggest that, despite a higher incidence of grade II acute GVHD in recipients of 2 partially HLA-matched UCB units, there is no adverse effect on TRM. This study is registered at (http://www.clinicaltrials.gov) under the identifiers NCT00305682 and NCT00309842.
Figures




References
-
- Weisdorf D, Haake R, Blazar B, et al. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: an analysis of clinical risk features and outcome. Blood. 1990;75:1024–1030. - PubMed
-
- Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: initial treatment. Blood. 1990;76:1464–1472. - PubMed
-
- Roy J, McGlave PB, Filipovich AH, et al. Acute graft-versus-host disease following unrelated donor marrow transplantation: failure of conventional therapy. Bone Marrow Transplant. 1992;10:77–82. - PubMed
-
- MacMillan ML, Weisdorf DJ, Wagner JE, et al. Response of 443 patients to steroids as primary therapy for acute graft-versus-host disease: comparison of grading systems. Biol Blood Marrow Transplant. 2002;8:387–394. - PubMed
-
- Kurtzberg J, Laughlin M, Graham ML, et al. Placental blood as a source of hematopoietic stem cells for transplantation into unrelated recipients. N Engl J Med. 1996;335:157–166. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
