

Vitamins E and C in the prevention of cardiovascular disease in men: the Physicians' Health Study II randomized controlled trial
- PMID: 18997197
- PMCID: PMC2586922
- DOI: 10.1001/jama.2008.600
Vitamins E and C in the prevention of cardiovascular disease in men: the Physicians' Health Study II randomized controlled trial
Abstract
Context: Basic research and observational studies suggest vitamin E or vitamin C may reduce the risk of cardiovascular disease. However, few long-term trials have evaluated men at initially low risk of cardiovascular disease, and no previous trial in men has examined vitamin C alone in the prevention of cardiovascular disease.
Objective: To evaluate whether long-term vitamin E or vitamin C supplementation decreases the risk of major cardiovascular events among men.
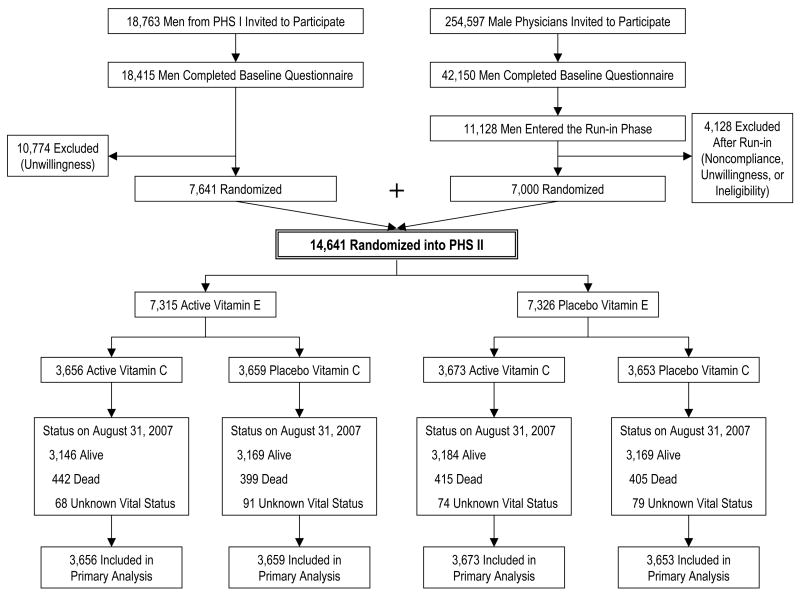
Design, setting, and participants: The Physicians' Health Study II was a randomized, double-blind, placebo-controlled factorial trial of vitamin E and vitamin C that began in 1997 and continued until its scheduled completion on August 31, 2007. There were 14,641 US male physicians enrolled, who were initially aged 50 years or older, including 754 men (5.1%) with prevalent cardiovascular disease at randomization.
Intervention: Individual supplements of 400 IU of vitamin E every other day and 500 mg of vitamin C daily.
Main outcome measures: A composite end point of major cardiovascular events (nonfatal myocardial infarction, nonfatal stroke, and cardiovascular disease death).
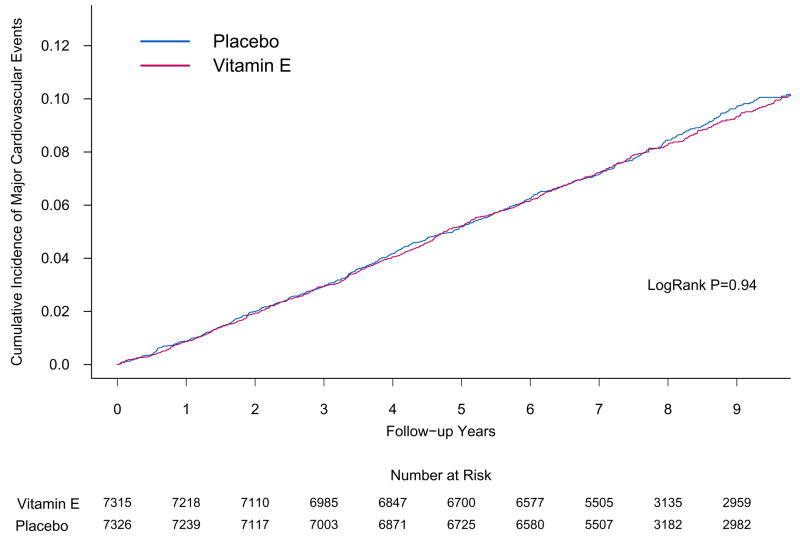
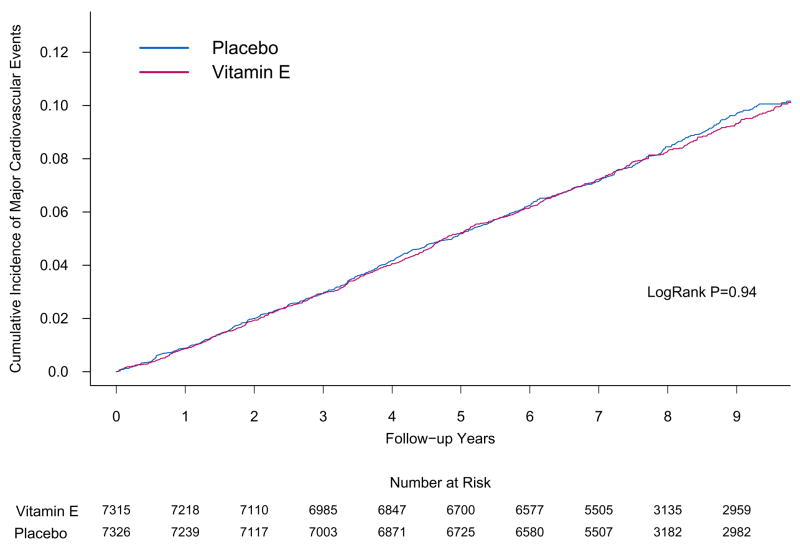
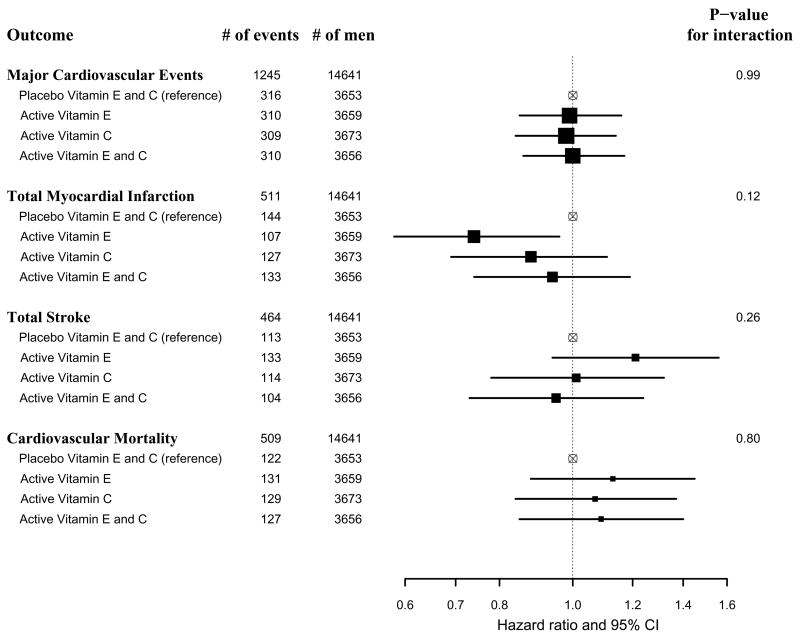
Results: During a mean follow-up of 8 years, there were 1245 confirmed major cardiovascular events. Compared with placebo, vitamin E had no effect on the incidence of major cardiovascular events (both active and placebo vitamin E groups, 10.9 events per 1000 person-years; hazard ratio [HR], 1.01 [95% confidence interval {CI}, 0.90-1.13]; P = .86), as well as total myocardial infarction (HR, 0.90 [95% CI, 0.75-1.07]; P = .22), total stroke (HR, 1.07 [95% CI, 0.89-1.29]; P = .45), and cardiovascular mortality (HR, 1.07 [95% CI, 0.90-1.28]; P = .43). There also was no significant effect of vitamin C on major cardiovascular events (active and placebo vitamin E groups, 10.8 and 10.9 events per 1000 person-years, respectively; HR, 0.99 [95% CI, 0.89-1.11]; P = .91), as well as total myocardial infarction (HR, 1.04 [95% CI, 0.87-1.24]; P = .65), total stroke (HR, 0.89 [95% CI, 0.74-1.07]; P = .21), and cardiovascular mortality (HR, 1.02 [95% CI, 0.85-1.21]; P = .86). Neither vitamin E (HR, 1.07 [95% CI, 0.97-1.18]; P = .15) nor vitamin C (HR, 1.07 [95% CI, 0.97-1.18]; P = .16) had a significant effect on total mortality but vitamin E was associated with an increased risk of hemorrhagic stroke (HR, 1.74 [95% CI, 1.04-2.91]; P = .04).
Conclusions: In this large, long-term trial of male physicians, neither vitamin E nor vitamin C supplementation reduced the risk of major cardiovascular events. These data provide no support for the use of these supplements for the prevention of cardiovascular disease in middle-aged and older men.
Trial registration: clinicaltrials.gov Identifier: NCT00270647.
Figures
Comment in
-
Vitamin E or vitamin C supplements did not differ from placebo for major cardiovascular events and mortality.Evid Based Nurs. 2009 Apr;12(2):48. doi: 10.1136/ebn.12.2.48. Evid Based Nurs. 2009. PMID: 19321825 No abstract available.
-
Antioxidant supplements and cardiovascular disease in men.JAMA. 2009 Apr 1;301(13):1335-6; author reply 1336-7. doi: 10.1001/jama.2009.315. JAMA. 2009. PMID: 19336703 No abstract available.
-
Antioxidant supplements and cardiovascular disease in men.JAMA. 2009 Apr 1;301(13):1335; author reply 1336-7. doi: 10.1001/jama.2009.314. JAMA. 2009. PMID: 19336704 No abstract available.
-
Antioxidant supplements and cardiovascular disease in men.JAMA. 2009 Apr 1;301(13):1336; author reply 1336-7. doi: 10.1001/jama.2009.316. JAMA. 2009. PMID: 19336705 Free PMC article. No abstract available.
-
ACP Journal Club. Supplementation with vitamin E or vitamin C did not differ from placebo for major cardiovascular events and mortality.Ann Intern Med. 2009 Apr 21;150(8):JC4-12. doi: 10.7326/0003-4819-150-8-200904210-02012. Ann Intern Med. 2009. PMID: 19391226 No abstract available.
References
-
- Timbo BB, Ross MP, McCarthy PV, Lin CT. Dietary supplements in a national survey: Prevalence of use and reports of adverse events. J Am Diet Assoc. 2006;106(12):1966–1974. - PubMed
-
- Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF. Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol. 2004;160(4):339–349. - PubMed
-
- Muth MK, Anderson DW, Domanico JL, Smith JB, Wendling B. Economic characterization of the dietary supplement industry. Washington DC: Center for Food Safety and Administration, Food and Drug Administration; 1999.
-
- Packer L. Protective role of vitamin E in biological systems. Am J Clin Nutr. 1991;53(4 Suppl):1050S–1055S. - PubMed
-
- Steinberg D, Lewis A. Conner Memorial Lecture. Oxidative modification of LDL and atherogenesis. Circulation. 1997;95(4):1062–1071. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
