

Toxicities associated with dual nucleoside reverse-transcriptase inhibitor regimens in HIV-infected children
- PMID: 19000014
- PMCID: PMC2737265
- DOI: 10.1086/593022
Toxicities associated with dual nucleoside reverse-transcriptase inhibitor regimens in HIV-infected children
Abstract
Background: Human immunodeficiency virus (HIV) therapy includes a backbone of nucleoside reverse-transcriptase inhibitors (NRTIs). Toxicities associated with NRTIs are not fully defined in children.
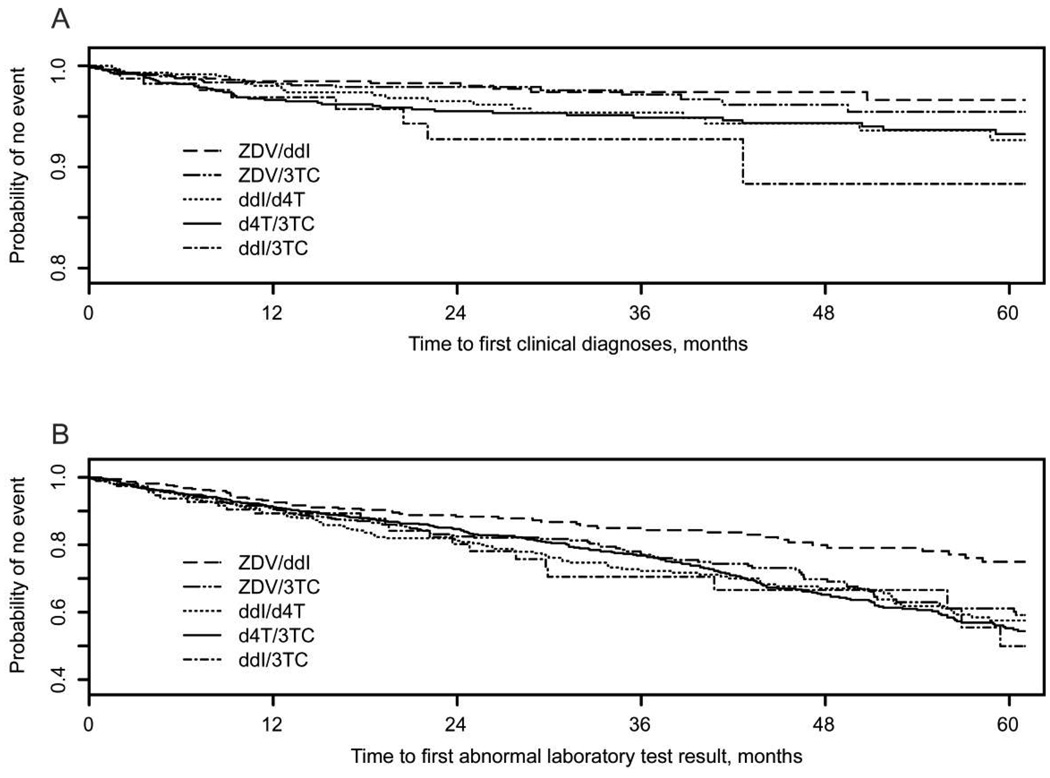
Methods: We studied 2233 children < or =13 years of age who were perinatally infected with HIV and were receiving > or =2 NRTIs, to determine the relative toxicities of the 5 most common NRTI pairs: zidovudine (ZDV)/lamivudine (3TC), ZDV/didanosine (ddI), stavudine (d4T)/3TC, d4T/ddI, and ddI/3TC. Incidence rates for clinical and laboratory toxicities were estimated, and NRTI pairs were compared with regard to the time to the first toxicity.
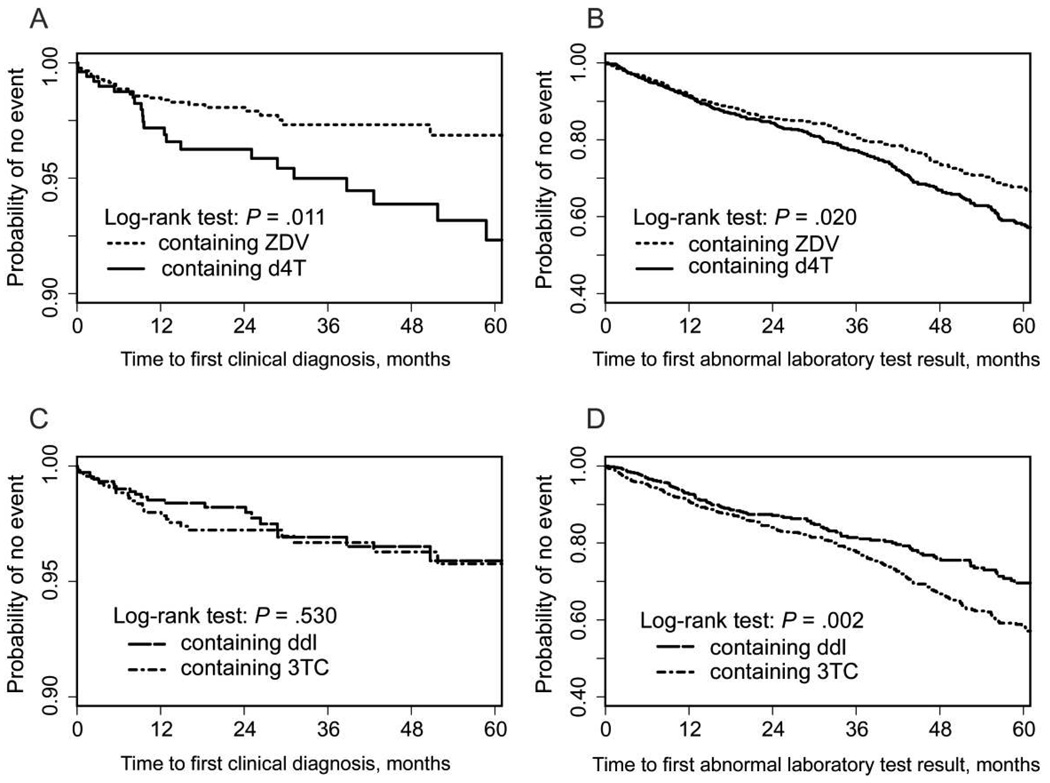
Results: The most common clinical toxicities noted were hepatitis, peripheral neuropathy, lipodystrophy/lipoatrophy, and pancreatitis, whereas the most common laboratory toxicities were an elevated anion gap, an increased total amylase level, neutropenia, and thrombocytopenia. Overall, regimens containing ZDV were associated with a significantly lower rate of clinical toxicities than were those containing d4T (adjusted hazard ratio [HR], 0.49; P = .02) ); regimens containing ddI were associated with a significantly lower rate of laboratory toxicities than were those containing 3TC (adjusted HR, 0.78; P = .04). ZDV/3TC was associated with a lower rate of clinical toxicities than were d4T/ddI and ddI/3TC and with a higher rate of laboratory toxicities than was ZDV/ddI. ZDV/ddI was associated with a lower rate of clinical toxicities than was d4T/3TC.
Conclusions: In children, regimens containing ZDV have less toxicity than do those containing d4T, thereby supporting their use in first-line regimens. D4T/3TC, d4T/ddI, and ddI/3TC have similar toxicity rates and are appropriate for second-line therapy.
Conflict of interest statement
Potential conflicts of interest: none reported.
Figures
References
-
- Brogly S, Williams P, Seage G, Oleske J, Van Dyke R, MacIntosh K for the PACTG 219C. Antiretroviral treatment in pediatric HIV in the United States: from clinical trials to clinical practice. JAMA. 2005;293:2213–2220. - PubMed
-
- Working Group on Antiretroviral Therapy and Medical Management of HIV-Infected Children. Guidelines for the use of antiretroviral agents in pediatric HIV infection. 2008. Feb 28 [Accessed 22 April 2008]. Available at: http://aidsinfo.nih.gov/ContentFiles/PediatricGuidelines.pdf. - PubMed
-
- Gortmaker S, Hughes M, Cervia J, et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001;345:1522–1528. - PubMed
-
- Ene L, Goetghebuer T, Hainaut M, et al. Prevalence of lipodystrophy in HIV-infected children: a cross-sectional study. Eur J Pediatr. 2007;166:13–21. - PubMed
-
- Department of Health and Human Services Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2008. Jan 29 [Accessed 22 April 2008]. Available at: http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI 068616/AI/NIAID NIH HHS/United States
- N01 HD033345/HD/NICHD NIH HHS/United States
- U01 AI068632/AI/NIAID NIH HHS/United States
- N01 HD 33345/HD/NICHD NIH HHS/United States
- M01 RR006192/RR/NCRR NIH HHS/United States
- U01 AI068616/AI/NIAID NIH HHS/United States
- U01 AI 068632/AI/NIAID NIH HHS/United States
- RR 05096/RR/NCRR NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- M01 RR005096/RR/NCRR NIH HHS/United States
- U01 AI041110/AI/NIAID NIH HHS/United States
- U01 AI 41110/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
