

Initial therapy of acute graft-versus-host disease with low-dose prednisone does not compromise patient outcomes
- PMID: 19001082
- PMCID: PMC2662636
- DOI: 10.1182/blood-2008-07-168401
Initial therapy of acute graft-versus-host disease with low-dose prednisone does not compromise patient outcomes
Abstract
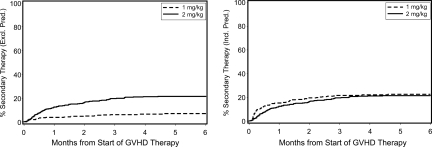
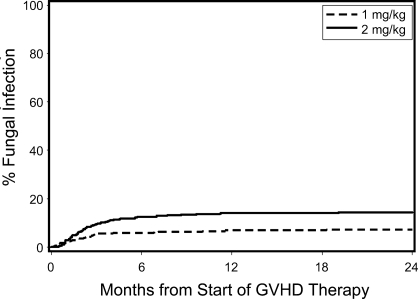
We hypothesized that initial treatment of acute graft-versus-host disease (GVHD) with low-dose glucocorticoids (prednisone-equivalent dose of 1 mg/kg per day) instead of standard-dose glucocorticoids (prednisone-equivalent dose of 2 mg/kg per day) does not compromise major transplantation outcomes. We retrospectively analyzed outcomes among 733 patients who received transplants between 2000 and 2005 according to initial treatment with low-dose (n=347) versus standard-dose (n=386) systemic glucocorticoids. The mean cumulative prednisone-equivalent doses at day 100 after starting treatment were 44 and 87 mg/kg for patients given low-dose and standard-dose glucocorticoids, respectively. Adjusted outcomes between the groups given low-dose versus standard-dose glucocorticoids were not statistically significantly different: overall mortality (hazard ratio [HR], 1.10; 95% confidence interval [CI], 0.9-1.4), relapse (HR, 1.22; 95% CI, 0.9-1.7), nonrelapse mortality (HR, 1.06; 95% CI, 0.8-1.5). The small number of patients with grades III/IV acute GVHD at onset precluded definitive conclusions for this subgroup. In multivariate analysis, the risks of invasive fungal infections (HR, 0.59; 95% CI, 0.3-1.0) and the duration of hospitalization (odds ratio, 0.62; 95% CI, 0.4-0.9) were reduced in the low-dose prednisone group. We conclude that initial treatment with low-dose glucocorticoids for patients with grades I-II GVHD did not compromise disease control or mortality and was associated with decreased toxicity.
Figures


Comment in
-
Where is the start line?Blood. 2009 Mar 26;113(13):2872-3. doi: 10.1182/blood-2008-12-192807. Blood. 2009. PMID: 19324908 No abstract available.
References
-
- Gratwohl A, Hermans J, Apperley J, et al. Acute graft-versus-host disease: grade and outcome in patients with chronic myelogenous leukemia [review]. Blood. 1995;86:813–818. - PubMed
-
- Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18:295–304. - PubMed
-
- Weisdorf D, Haake R, Blazar B, et al. Treatment of moderate/severe acute graft-versus-host disease after allogeneic bone marrow transplantation: an analysis of clinical risk features and outcome. Blood. 1990;75:1024–1030. - PubMed
-
- Shlomchik WD. Graft-versus-host disease. Nat Rev Immunol. 2007;7:340–352. - PubMed
-
- Storb R, Deeg HJ, Whitehead J, et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med. 1986;314:729–735. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA18029/CA/NCI NIH HHS/United States
- HL36444/HL/NHLBI NIH HHS/United States
- CA92058/CA/NCI NIH HHS/United States
- CA09515/CA/NCI NIH HHS/United States
- CA15704/CA/NCI NIH HHS/United States
- T32 CA009515/CA/NCI NIH HHS/United States
- U10 CA180828/CA/NCI NIH HHS/United States
- P01 HL036444/HL/NHLBI NIH HHS/United States
- P01 CA078902/CA/NCI NIH HHS/United States
- P01 CA018029/CA/NCI NIH HHS/United States
- P30 CA015704/CA/NCI NIH HHS/United States
- CA78902/CA/NCI NIH HHS/United States
- K23 CA092058/CA/NCI NIH HHS/United States
- CA18221/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
