

Frequent amyloid deposition without significant cognitive impairment among the elderly
- PMID: 19001171
- PMCID: PMC2636844
- DOI: 10.1001/archneur.65.11.1509
Frequent amyloid deposition without significant cognitive impairment among the elderly
Abstract
Objective: To characterize the prevalence of amyloid deposition in a clinically unimpaired elderly population, as assessed by Pittsburgh Compound B (PiB) positron emission tomography (PET) imaging, and its relationship to cognitive function, measured with a battery of neuropsychological tests.
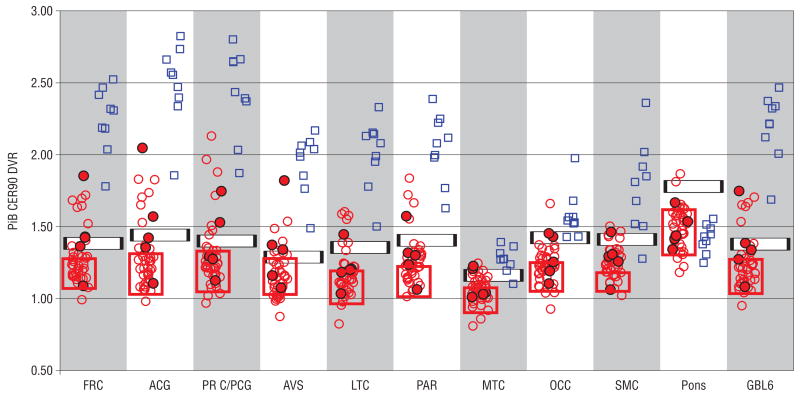
Design: Subjects underwent cognitive testing and PiB PET imaging (15 mCi for 90 minutes with an ECAT HR+ scanner). Logan graphical analysis was applied to estimate regional PiB retention distribution volume, normalized to a cerebellar reference region volume, to yield distribution volume ratios (DVRs).
Setting: University medical center.
Participants: From a community-based sample of volunteers, 43 participants aged 65 to 88 years who did not meet diagnostic criteria for Alzheimer disease or mild cognitive impairment were included.
Main outcome measures: Regional PiB retention and cognitive test performance.
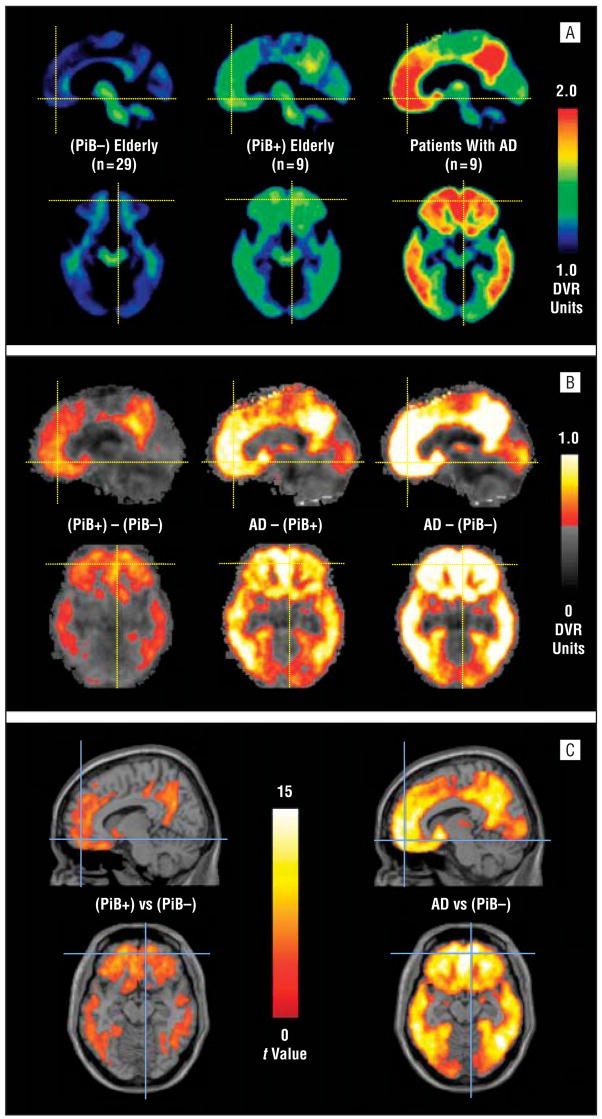
Results: Of 43 clinically unimpaired elderly persons imaged, 9 (21%) showed evidence of early amyloid deposition in at least 1 brain area using an objectively determined DVR cutoff. Demographic characteristics did not differ significantly between amyloid-positive and amyloid-negative participants, and neurocognitive performance was not significantly worse among amyloid-positive compared with amyloid-negative participants.
Conclusions: Amyloid deposition can be identified among cognitively normal elderly persons during life, and the prevalence of asymptomatic amyloid deposition may be similar to that of symptomatic amyloid deposition. In this group of participants without clinically significant impairment, amyloid deposition was not associated with worse cognitive function, suggesting that an elderly person with a significant amyloid burden can remain cognitively normal. However, this finding is based on relatively small numbers and needs to be replicated in larger cohorts. Longitudinal follow-up of these subjects will be required to support the potential of PiB imaging to identify preclinical Alzheimer disease, or, alternatively, to show that amyloid deposition is not sufficient to cause Alzheimer disease within some specified period.
Figures
Comment in
-
Substantial amyloid deposition without cognitive impairment.Nat Clin Pract Neurol. 2009 Mar;5(3):123. Nat Clin Pract Neurol. 2009. PMID: 20408269 No abstract available.
References
-
- Dickson DW, Crystal HA, Mattiace LA, et al. Identification of normal and pathological aging in prospectively studied nondemented elderly humans. Neurobiol Aging. 1992;13(1):179–189. - PubMed
-
- Haroutunian V, Perl D, Purohit D, et al. Regional distribution of neuritic plaques in the nondemented elderly and subjects with very mild Alzheimer’s disease. Arch Neurol. 1998;55(9):1185–1191. - PubMed
-
- Price JL, Morris JC. Tangles and plaques in nondemented aging and “preclinical” Alzheimer’s disease. Ann Neurol. 1999;45(3):358–368. - PubMed
-
- Wolf DS, Gearing M, Snowdon DA, Mori H, Markesbery WR, Mirra SS. Progression of regional neuropathology in Alzheimer disease and normal elderly: findings from the Nun Study. Alzheimer Dis Assoc Disord. 1999;13(4):226–231. - PubMed
-
- Lopez OL, Jagust WJ, DeKosky ST, et al. Prevalence and classification of mild cognitive impairment in the Cardiovascular Health Study Cognition Study: part 1. Arch Neurol. 2003;60(10):1385–1389. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
