

FDG-PET/MRI coregistration improves detection of cortical dysplasia in patients with epilepsy
- PMID: 19001249
- PMCID: PMC2676967
- DOI: 10.1212/01.wnl.0000334752.41807.2f
FDG-PET/MRI coregistration improves detection of cortical dysplasia in patients with epilepsy
Abstract
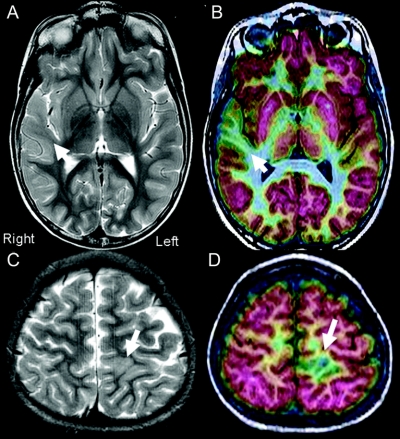
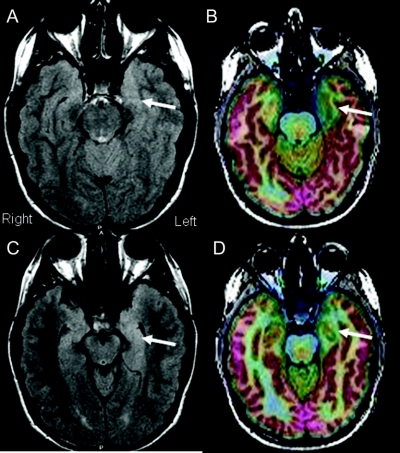
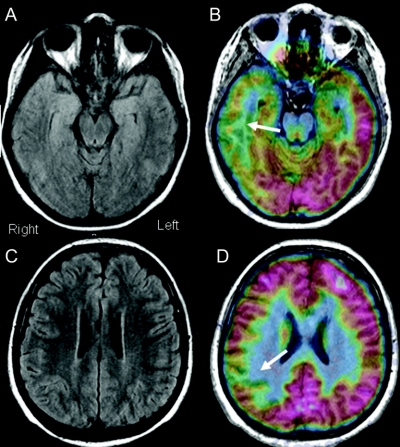
Objective: Patients with cortical dysplasia (CD) are difficult to treat because the MRI abnormality may be undetectable. This study determined whether fluorodeoxyglucose (FDG)-PET/MRI coregistration enhanced the recognition of CD in epilepsy surgery patients.
Methods: Patients from 2004-2007 in whom FDG-PET/MRI coregistration was a component of the presurgical evaluation were compared with patients from 2000-2003 without this technique. For the 2004-2007 cohort, neuroimaging and clinical variables were compared between patients with mild Palmini type I and severe Palmini type II CD.
Results: Compared with the 2000-2003 cohort, from 2004-2007 more CD patients were detected, most had type I CD, and fewer cases required intracranial electrodes. From 2004-2007, 85% of type I CD cases had normal non-University of California, Los Angeles (UCLA) MRI scans. UCLA MRI identified CD in 78% of patients, and 37% of type I CD cases had normal UCLA scans. EEG and neuroimaging findings were concordant in 52% of type I CD patients, compared with 89% of type II CD patients. FDG-PET scans were positive in 71% of CD cases, and type I CD patients had less hypometabolism compared with type II CD patients. Postoperative seizure freedom occurred in 82% of patients, without differences between type I and type II CD cases.
Conclusions: Incorporating fluorodeoxyglucose-PET/MRI coregistration into the multimodality presurgical evaluation enhanced the noninvasive identification and successful surgical treatment of patients with cortical dysplasia (CD), especially for the 33% of patients with nonconcordant findings and those with normal MRI scans from mild type I CD.
Figures
Comment in
-
Cortical dyplasia: complete resection correlates with outcome ... But, complete resection of what?Epilepsy Curr. 2009 Jul-Aug;9(4):100-2. doi: 10.1111/j.1535-7511.2009.01306.x. Epilepsy Curr. 2009. PMID: 19693325 Free PMC article. No abstract available.
References
-
- Becker AJ, Blumcke I, Urbach H, Hans V, Majores M. Molecular neuropathology of epilepsy-associated glioneuronal malformations. J Neuropathol Exp Neurol 2006;65:99–108. - PubMed
-
- Harvey AS, Cross JH, Shinnar S, Mathern BW. Defining the spectrum of international practice in pediatric epilepsy surgery patients. Epilepsia 2008;49:146–155. - PubMed
-
- Mischel PS, Nguyen LP, Vinters HV. Cerebral cortical dysplasia associated with pediatric epilepsy: review of neuropathologic features and proposal for a grading system. J Neuropathol Exp Neurol 1995;54:137–153. - PubMed
-
- Palmini A, Najm I, Avanzini G, et al. Terminology and classification of the cortical dysplasias. Neurology 2004;62 (suppl 3):S2–S8. - PubMed