

Detection of paroxysmal nocturnal hemoglobinuria clones in patients with myelodysplastic syndromes and related bone marrow diseases, with emphasis on diagnostic pitfalls and caveats
- PMID: 19001281
- PMCID: PMC2625410
- DOI: 10.3324/haematol.13601
Detection of paroxysmal nocturnal hemoglobinuria clones in patients with myelodysplastic syndromes and related bone marrow diseases, with emphasis on diagnostic pitfalls and caveats
Abstract
Background: The presence of paroxysmal nocturnal hemoglobinuria clones in the setting of aplastic anemia or myelodysplastic syndrome has been shown to have prognostic and therapeutic implications. However, the status of paroxysmal nocturnal hemoglobinuria clones in various categories of myelodysplastic syndrome and in other bone marrow disorders is not well-studied.
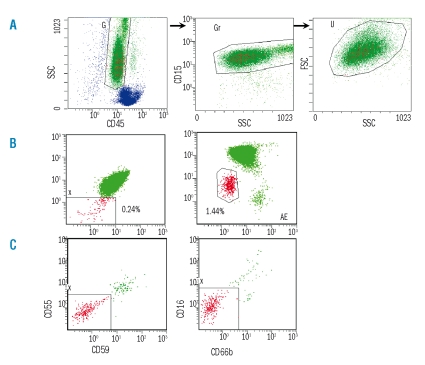
Design and methods: By using multiparameter flow cytometry immunophenotypic analysis with antibodies specific for four glycosylphosphatidylinositol-anchored proteins (CD55, CD59, CD16, CD66b) and performing an aerolysin lysis confirmatory test in representative cases, we assessed the paroxysmal nocturnal hemoglobinuria-phenotype granulocytes in 110 patients with myelodysplastic syndrome, 15 with myelodysplastic/myeloproliferative disease, 5 with idiopathic myelofibrosis and 6 with acute myeloid leukemia.
Results: Paroxysmal nocturnal hemoglobinuria-phenotype granulocytes were detected in nine patients with low grade myelodysplastic syndrome who showed clinicopathological features of bone marrow failure, similar to aplastic anemia. All paroxysmal nocturnal hemoglobinuria-positive cases demonstrated loss of the four glycosylphosphatidylinositol-anchored proteins, with CD16(-)CD66b(-) clones being larger than those of CD55(-)CD59(-) (p<0.05). Altered glycosylphosphatidylinositol-anchored protein expression secondary to granulocytic hypogranulation, immaturity, and/or immunophenotypic abnormalities was present in a substantial number of cases and diagnostically challenging.
Conclusions: These results show that routine screening for paroxysmal nocturnal hemoglobinuria clones in patients with an intrinsic bone marrow disease who show no clinical evidence of hemolysis has an appreciable yield in patients with low grade myelodysplastic syndromes. The recognition of diagnostic caveats and pitfalls associated with the underlying intrinsic bone marrow disease is essential in interpreting paroxysmal nocturnal hemoglobinuria testing correctly. In our experience, the CD16/CD66b antibody combination is superior to CD55/CD59 in screening for subclinical paroxysmal nocturnal hemoglobinuria because it detects a large clone size and is less subject to analytical interference.
Figures

Comment in
-
Paroxysmal nocturnal hemoglobinuria and myelodysplastic syndromes: clonal expansion of PIG-A-mutant hematopoietic cells in bone marrow failure.Haematologica. 2009 Jan;94(1):3-7. doi: 10.3324/haematol.2008.001297. Haematologica. 2009. PMID: 19118373 Free PMC article.
Similar articles
-
Value of CD16/CD66b/CD45 in comparison to CD55/CD59/CD45 in diagnosis of paroxysmal nocturnal haemoglobinuria: An Indian experience.Indian J Med Res. 2017 Sep;146(3):362-368. doi: 10.4103/ijmr.IJMR_195_14. Indian J Med Res. 2017. PMID: 29355143 Free PMC article.
-
Impaired hematopoiesis in paroxysmal nocturnal hemoglobinuria/aplastic anemia is not associated with a selective proliferative defect in the glycosylphosphatidylinositol-anchored protein-deficient clone.Blood. 1997 Feb 15;89(4):1173-81. Blood. 1997. PMID: 9028939
-
Paroxysmal nocturnal hemoglobinuria cells in patients with bone marrow failure syndromes.Ann Intern Med. 1999 Sep 21;131(6):401-8. doi: 10.7326/0003-4819-131-6-199909210-00002. Ann Intern Med. 1999. PMID: 10498555
-
Paroxysmal nocturnal hemoglobinuria in children.Paediatr Drugs. 2007;9(1):11-6. doi: 10.2165/00148581-200709010-00002. Paediatr Drugs. 2007. PMID: 17291133 Review.
-
[Anemia with aplastic anemia, paroxysmal nocturnal hemoglobinuria and myelodysplastic syndromes].Ther Umsch. 2010 May;67(5):251-5. doi: 10.1024/0040-5930/a000045. Ther Umsch. 2010. PMID: 20509122 Review. German.
Cited by
-
Flow Cytometric Diagnosis of Paroxysmal Nocturnal Hemoglobinuria: Pearls and Pitfalls - A Critical Review Article.EJIFCC. 2019 Nov 25;30(4):355-370. eCollection 2019 Nov. EJIFCC. 2019. PMID: 31814811 Free PMC article. Review.
-
FLAER Based Assay According to Newer Guidelines Increases Sensitivity of PNH Clone Detection.Indian J Hematol Blood Transfus. 2020 Jul;36(3):526-534. doi: 10.1007/s12288-019-01220-8. Epub 2019 Nov 5. Indian J Hematol Blood Transfus. 2020. PMID: 32647428 Free PMC article.
-
Frequency of paroxysmal nocturnal hemoglobinuria in patients attended in Belém, Pará, Brazil.Rev Bras Hematol Hemoter. 2011;33(1):35-7. doi: 10.5581/1516-8484.20110012. Rev Bras Hematol Hemoter. 2011. PMID: 23284241 Free PMC article.
-
Assay sensitivity of flow cytometric PNH analysis: response to Brando and Gatti.Ann Hematol. 2022 Feb;101(2):461-464. doi: 10.1007/s00277-021-04478-z. Epub 2021 Apr 27. Ann Hematol. 2022. PMID: 33904954 No abstract available.
-
Copper deficiency with 20q deletion and a paroxysmal nocturnal haemoglobinuria clone presenting with bicytopenia.Indian J Hematol Blood Transfus. 2014 Sep;30(Suppl 1):372-5. doi: 10.1007/s12288-014-0419-8. Epub 2014 Jun 13. Indian J Hematol Blood Transfus. 2014. PMID: 25332623 Free PMC article.
References
-
- Takeda J, Miyata T, Kawagoe K, Iida Y, Endo Y, Fujita T, et al. Deficiency of the GPI anchor caused by a somatic mutation of the PIG-A gene in paroxysmal nocturnal hemoglobinuria. Cell. 1993;73:703–11. - PubMed
-
- Griscelli-Bennaceur A, Gluckman E, Scrobohaci ML, Jonveaux P, Vu T, Bazarbachi A, et al. Aplastic anemia and paroxysmal nocturnal hemoglobinuria: search for a pathogenetic link. Blood. 1995;85:1354–63. - PubMed
-
- Schubert J, Vogt HG, Zielinska-Skowronek M, Freund M, Kaltwasser JP, Hoelzer D, et al. Development of the glycosylphosphatidylinositol-anchoring defect characteristic for paroxysmal nocturnal hemoglobinuria in patients with aplastic anemia. Blood. 1994;83:2323–8. - PubMed
-
- Maciejewski JP, Rivera C, Kook H, Dunn D, Young NS. Relationship between bone marrow failure syndromes and the presence of glycophosphatidylinositol-anchored protein-deficient clones. Br J Haematol. 2001;115:1015–22. - PubMed
-
- Wang H, Chuhjo T, Yasue S, Omine M, Nakao S. Clinical significance of a minor population of paroxysmal nocturnal hemoglobinuria-type cells in bone marrow failure syndrome. Blood. 2002;100:3897–902. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
