

Mechanical ventilation guided by esophageal pressure in acute lung injury
- PMID: 19001507
- PMCID: PMC3969885
- DOI: 10.1056/NEJMoa0708638
Mechanical ventilation guided by esophageal pressure in acute lung injury
Abstract
Background: Survival of patients with acute lung injury or the acute respiratory distress syndrome (ARDS) has been improved by ventilation with small tidal volumes and the use of positive end-expiratory pressure (PEEP); however, the optimal level of PEEP has been difficult to determine. In this pilot study, we estimated transpulmonary pressure with the use of esophageal balloon catheters. We reasoned that the use of pleural-pressure measurements, despite the technical limitations to the accuracy of such measurements, would enable us to find a PEEP value that could maintain oxygenation while preventing lung injury due to repeated alveolar collapse or overdistention.
Methods: We randomly assigned patients with acute lung injury or ARDS to undergo mechanical ventilation with PEEP adjusted according to measurements of esophageal pressure (the esophageal-pressure-guided group) or according to the Acute Respiratory Distress Syndrome Network standard-of-care recommendations (the control group). The primary end point was improvement in oxygenation. The secondary end points included respiratory-system compliance and patient outcomes.
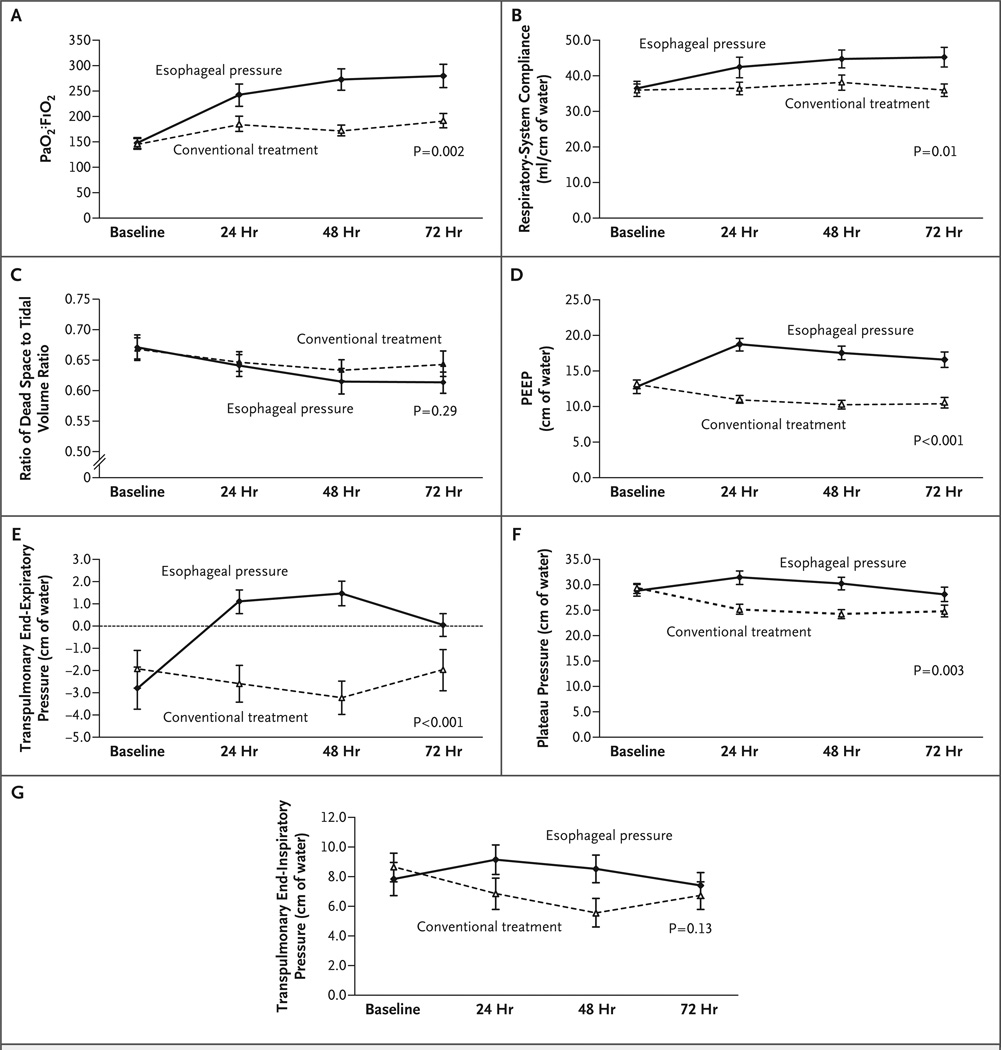
Results: The study reached its stopping criterion and was terminated after 61 patients had been enrolled. The ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen at 72 hours was 88 mm Hg higher in the esophageal-pressure-guided group than in the control group (95% confidence interval, 78.1 to 98.3; P=0.002). This effect was persistent over the entire follow-up time (at 24, 48, and 72 hours; P=0.001 by repeated-measures analysis of variance). Respiratory-system compliance was also significantly better at 24, 48, and 72 hours in the esophageal-pressure-guided group (P=0.01 by repeated-measures analysis of variance).
Conclusions: As compared with the current standard of care, a ventilator strategy using esophageal pressures to estimate the transpulmonary pressure significantly improves oxygenation and compliance. Multicenter clinical trials are needed to determine whether this approach should be widely adopted. (ClinicalTrials.gov number, NCT00127491.)
2008 Massachusetts Medical Society
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures

Comment in
-
PEEP guided by esophageal pressure--any added value?N Engl J Med. 2008 Nov 13;359(20):2166-8. doi: 10.1056/NEJMe0806637. Epub 2008 Nov 11. N Engl J Med. 2008. PMID: 19001506 No abstract available.
-
Esophageal pressure in acute lung injury.N Engl J Med. 2009 Feb 19;360(8):831; author reply 832-3. doi: 10.1056/NEJMc082492. N Engl J Med. 2009. PMID: 19228629 No abstract available.
-
Esophageal pressure in acute lung injury.N Engl J Med. 2009 Feb 19;360(8):831-2; author reply 832-3. N Engl J Med. 2009. PMID: 19238672 No abstract available.
-
Esophageal pressure in acute lung injury.N Engl J Med. 2009 Feb 19;360(8):832; author reply 832-3. N Engl J Med. 2009. PMID: 19238673 No abstract available.
-
Esophageal pressure in acute lung injury.N Engl J Med. 2009 Feb 19;360(8):832; author reply 832-3. N Engl J Med. 2009. PMID: 19238674 No abstract available.
-
The esophagus ... not just for food anymore?Crit Care. 2010;14(6):326. doi: 10.1186/cc9314. Epub 2010 Nov 5. Crit Care. 2010. PMID: 21092152 Free PMC article. No abstract available.
References
-
- Brower RG, Lanken PN, MacIntyre N, et al. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med. 2004;351:327–336. - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299:637–645. - PubMed
-
- Mercat A, Richard JC, Vielle B, et al. Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299:646–655. - PubMed
-
- Grasso S, Fanelli V, Cafarelli A, et al. Effects of high versus low positive end-expiratory pressures in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2005;171:1002–1008. - PubMed
-
- Slutsky AS. Lung injury caused by mechanical ventilation. Chest. 1999;116(Suppl):9S–15S. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials