

MR imaging detection of cerebral microbleeds: effect of susceptibility-weighted imaging, section thickness, and field strength
- PMID: 19001544
- PMCID: PMC2760298
- DOI: 10.3174/ajnr.A1355
MR imaging detection of cerebral microbleeds: effect of susceptibility-weighted imaging, section thickness, and field strength
Abstract
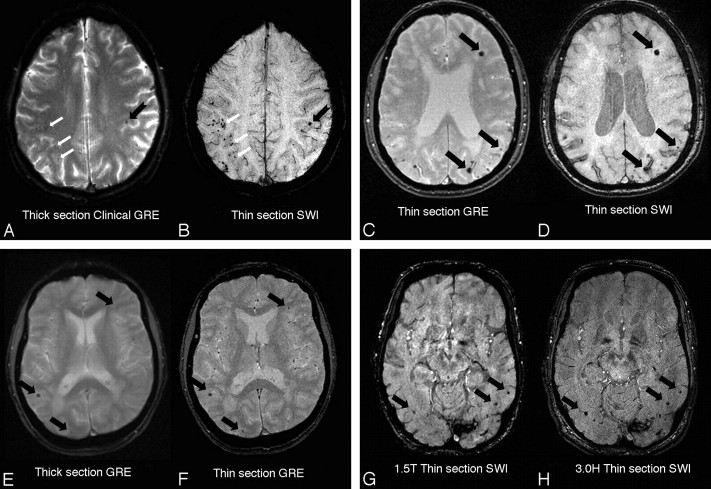
Background and purpose: The emergence of cerebral microbleeds (CMB) as common MR imaging findings raises the question of how MR imaging parameters influence CMB detection. To evaluate the effects of modified gradient recalled-echo (GRE) MR imaging methods, we performed an analysis of sequence, section thickness, and field strength on CMB imaging properties and detection in subjects with cerebral amyloid angiopathy (CAA), a condition associated with microhemorrhage.
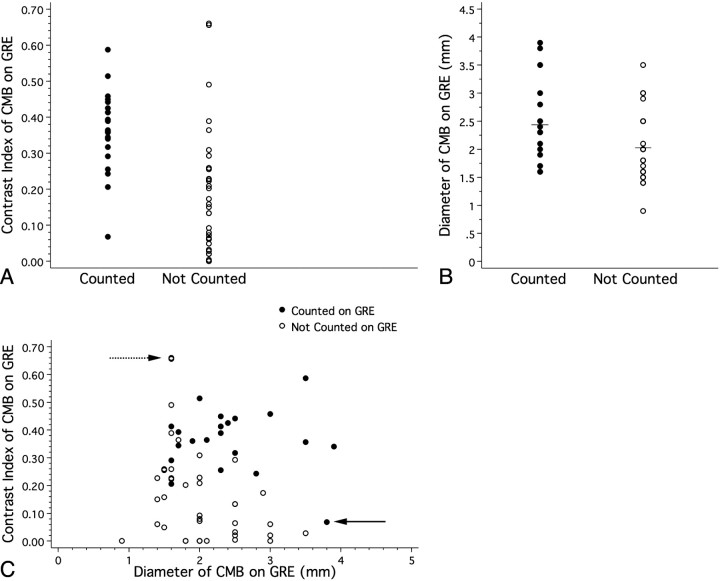
Materials and methods: Multiple MR images were obtained from subjects with probable CAA, with varying sequences (GRE versus susceptibility-weighted imaging [SWI]), section thicknesses (1.2-1.5 versus 5 mm), and magnetic field strengths (1.5T versus 3T). Individual CMB were manually identified and analyzed for contrast index (lesion intensity normalized to normal-appearing white matter signal intensity) and diameter. CMB counts were compared between 1.5T thick-section GRE and thin-section SWI for 3 subjects who underwent both protocols in the same scanning session.
Results: With other parameters constant, use of SWI, thinner sections, and a higher field strength yielded medium-to-large gains in CMB contrast index (CI; Cohen d 0.71-1.87). SWI was also associated with small increases in CMB diameter (Cohen d <0.3). Conventional thick-section GRE identified only 33% of CMB (103 of 310) seen on thin-section SWI. Lesions prospectively identified on GRE had significantly greater CI and diameter measured on the GRE image than those not prospectively identified.
Conclusions: The examined alternatives to conventional GRE MR imaging yield substantially improved CMB contrast and sensitivity for detection. Future studies based on these techniques will most likely yield even higher prevalence estimates for CMB.
Figures
Similar articles
-
Susceptibility-weighted imaging is more reliable than T2*-weighted gradient-recalled echo MRI for detecting microbleeds.Stroke. 2013 Oct;44(10):2782-6. doi: 10.1161/STROKEAHA.113.002267. Epub 2013 Aug 6. Stroke. 2013. PMID: 23920014 Clinical Trial.
-
SWI or T2*: which MRI sequence to use in the detection of cerebral microbleeds? The Karolinska Imaging Dementia Study.AJNR Am J Neuroradiol. 2015 Jun;36(6):1089-95. doi: 10.3174/ajnr.A4248. Epub 2015 Feb 19. AJNR Am J Neuroradiol. 2015. PMID: 25698623 Free PMC article.
-
SWI versus GRE-T2*: Assessing cortical superficial siderosis in advanced cerebral amyloid angiopathy.Rev Neurol (Paris). 2024 Jun;180(6):532-538. doi: 10.1016/j.neurol.2023.10.008. Epub 2023 Dec 6. Rev Neurol (Paris). 2024. PMID: 38061969
-
Cerebral microbleeds on MRI: prevalence, associations, and potential clinical implications.Neurology. 2006 Jan 24;66(2):165-71. doi: 10.1212/01.wnl.0000194266.55694.1e. Neurology. 2006. PMID: 16434647 Review.
-
Cerebral microbleed detection and mapping: principles, methodological aspects and rationale in vascular dementia.Exp Gerontol. 2012 Nov;47(11):843-52. doi: 10.1016/j.exger.2012.06.008. Epub 2012 Jun 29. Exp Gerontol. 2012. PMID: 22750456 Review.
Cited by
-
Susceptibility weighted imaging: a new tool in the diagnosis of prostate cancer and detection of prostatic calcification.PLoS One. 2013;8(1):e53237. doi: 10.1371/journal.pone.0053237. Epub 2013 Jan 7. PLoS One. 2013. PMID: 23308170 Free PMC article.
-
Comparison of ESWAN, SWI-SPGR, and 2D T2*-weighted GRE sequence for depicting cerebral microbleeds.Clin Neuroradiol. 2013 Jun;23(2):121-7. doi: 10.1007/s00062-012-0185-7. Epub 2012 Dec 3. Clin Neuroradiol. 2013. PMID: 23212660
-
Radiological assessment of dementia: the Italian inter-society consensus for a practical and clinically oriented guide to image acquisition, evaluation, and reporting.Radiol Med. 2022 Sep;127(9):998-1022. doi: 10.1007/s11547-022-01534-0. Epub 2022 Sep 7. Radiol Med. 2022. PMID: 36070064 Free PMC article.
-
Predicting cerebral amyloid angiopathy-related intracerebral hemorrhages and other cerebrovascular disorders in Alzheimer's disease.Front Neurol. 2012 Apr 25;3:64. doi: 10.3389/fneur.2012.00064. eCollection 2012. Front Neurol. 2012. PMID: 22539931 Free PMC article.
-
Lewy body pathology modifies risk factors for cerebral amyloid angiopathy when comorbid with Alzheimer's disease pathology.Alzheimers Dement. 2024 Apr;20(4):2564-2574. doi: 10.1002/alz.13704. Epub 2024 Feb 14. Alzheimers Dement. 2024. PMID: 38353367 Free PMC article.
References
-
- Jeerakathil T, Wolf PA, Beiser A, et al. Cerebral microbleeds: prevalence and associations with cardiovascular risk factors in the Framingham Study. Stroke 2004;35:1831–35. Epub 2004 May 20 - PubMed
-
- Koennecke HC. Cerebral microbleeds on MRI: prevalence, associations, and potential clinical implications. Neurology 2006;66:165–71 - PubMed
-
- Viswanathan A, Chabriat H. Cerebral microhemorrhage. Stroke 2006;37:550–55 - PubMed
-
- Cordonnier C, Al-Shahi Salman R, Wardlaw J. Spontaneous brain microbleeds: systematic review, subgroup analyses and standards for study design and reporting. Brain 2007;130:1988–2003 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical