

Pancreatic adenocarcinoma patients with localised chronic severe pancreatitis show an increased number of single beta cells, without alterations in fractional insulin area
- PMID: 19002428
- PMCID: PMC7321839
- DOI: 10.1007/s00125-008-1200-z
Pancreatic adenocarcinoma patients with localised chronic severe pancreatitis show an increased number of single beta cells, without alterations in fractional insulin area
Abstract
Aims/hypothesis: Recent histological analysis of pancreases obtained from patients with long-standing type 1 diabetes identified chronic islet inflammation and limited evidence suggestive of beta cell replication. Studies in rodent models also suggest that beta cell replication can be induced by certain inflammatory cytokines and by gastrin. We therefore tested the hypothesis that beta cell replication is observed in non-autoimmune human pancreatic disorders in which localised inflammation or elevated gastrin levels are present.
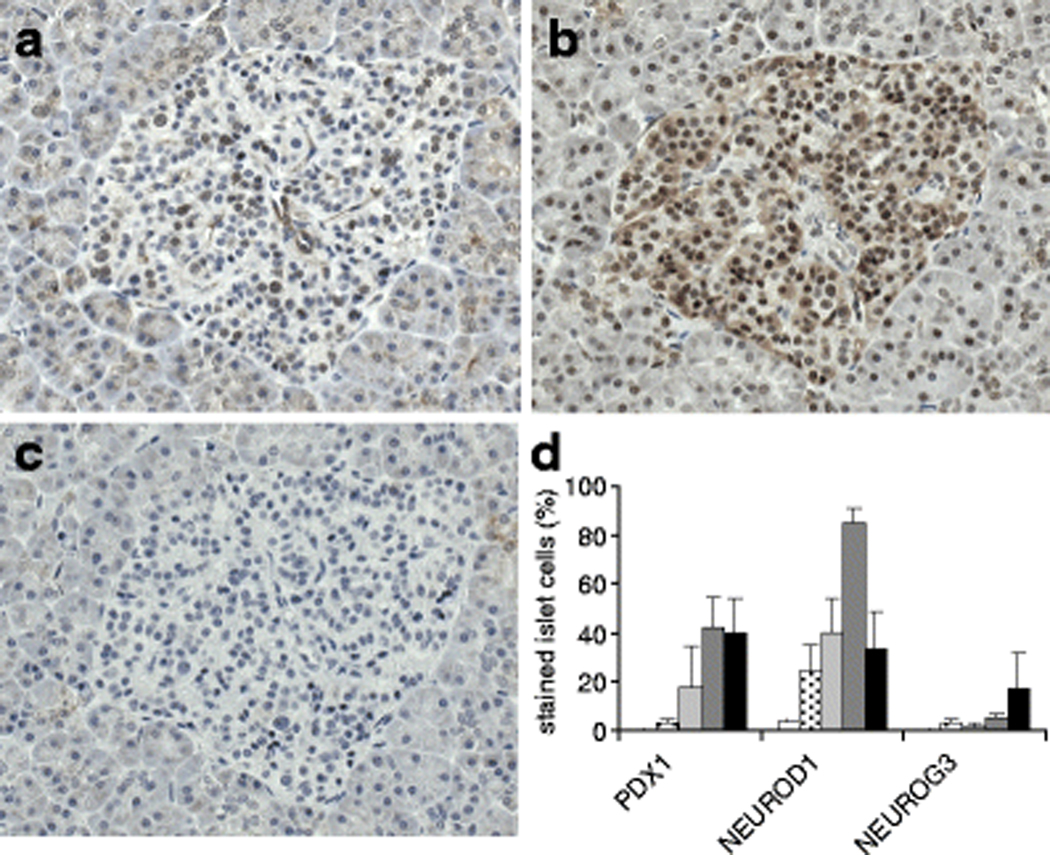
Methods: Resected operative pancreatic specimens were obtained from patients diagnosed with primary adenocarcinoma (with or without chronic severe pancreatitis) or gastrinoma. Additional pancreatic tissue was obtained from autopsy control patients. Immunohistochemistry was used to assess fractional insulin area, beta cell number and replication rate and differentiation factors relevant to beta cell development.
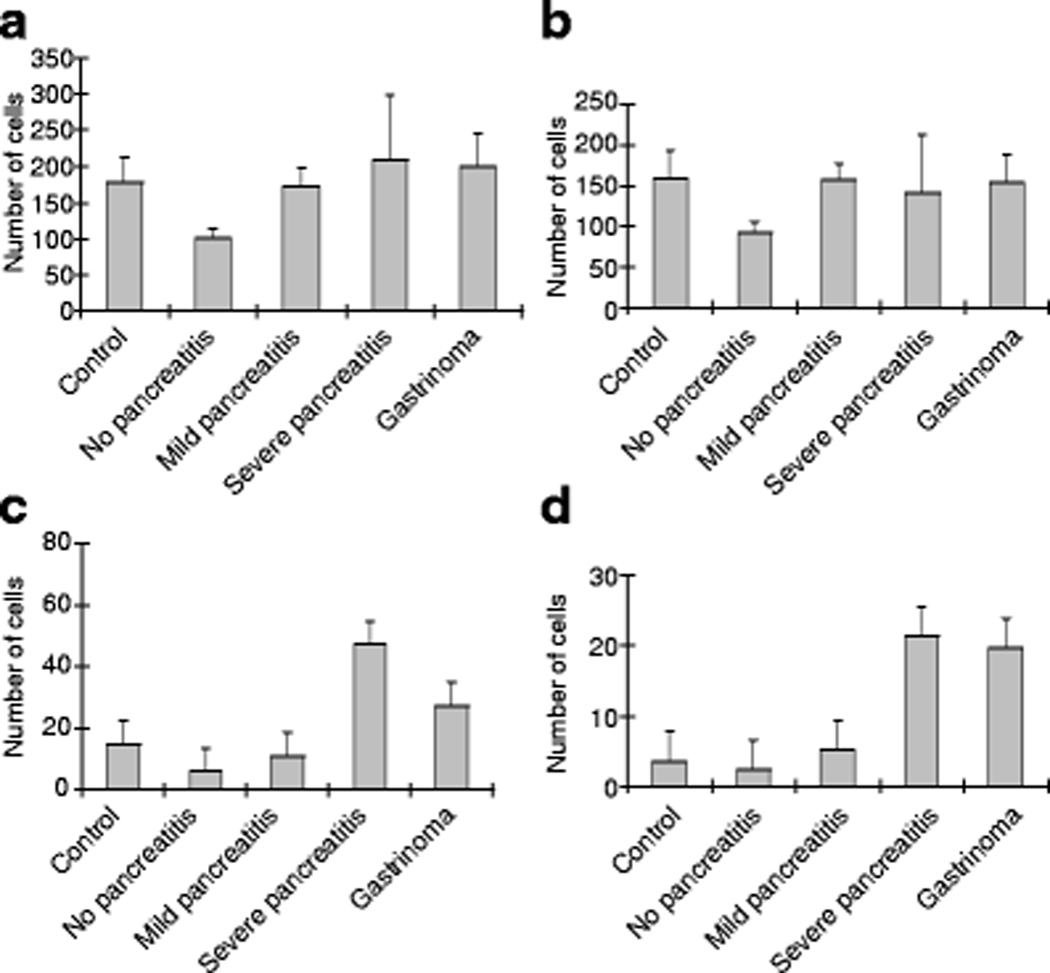
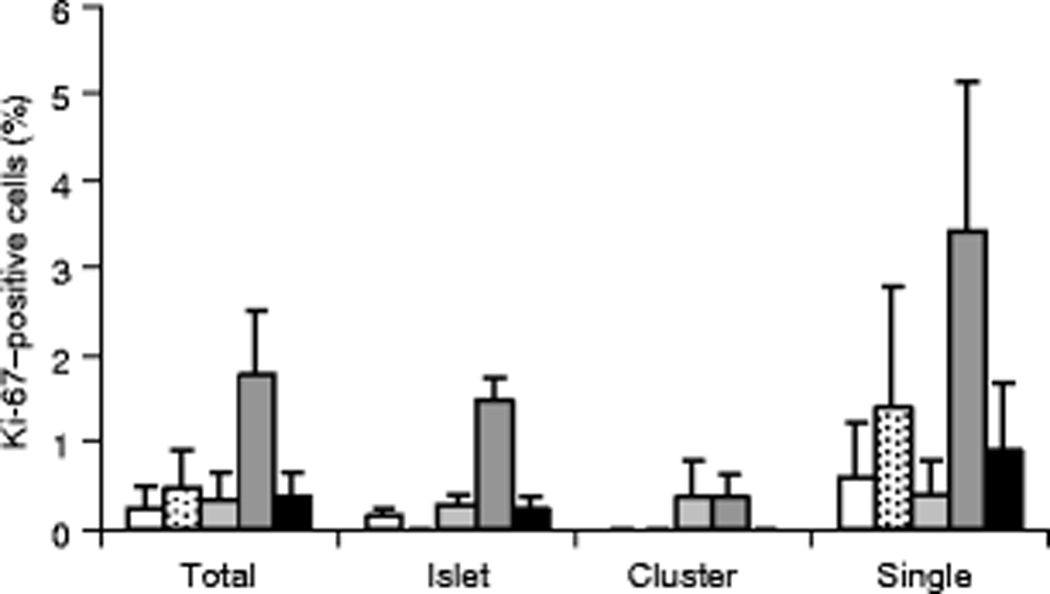
Results: Fractional insulin area was similar among groups. Patients with pancreatic adenocarcinoma and localised chronic severe pancreatitis displayed significant increases in the number of single beta cells, as well as increased beta cell replication rate and levels of neurogenic differentiation 1 in islets. Patients with gastrinoma demonstrated significant increases in the number of single beta cells, but the beta cell replication rate and islet differentiation factor levels were similar to those in the control group.
Conclusions/interpretation: These findings indicate that chronic severe pancreatic inflammation can be associated with significant effects on beta cell number or replication rate, depending on the distribution of the cells. This information may prove useful for attempts seeking to design therapies aimed at inducing beta cell replication as a means of reversing diabetes.
Figures


References
-
- Atkinson MA, Rhodes CJ (2005) Pancreatic regeneration in type 1 diabetes: dreams on a deserted islet? Diabetologia 48: 2200–2202 - PubMed
-
- Meier JJ, Bhushan A, Butler AE, Rizza RA, Butler PC (2005) Sustained beta cell apoptosis in patients with long-standing type 1 diabetes: indirect evidence for islet regeneration? Diabetologia 48: 2221–2228 - PubMed
-
- Bonner-Weir S, Weir GC (2005) New sources of pancreatic beta-cells. Nat Biotechnol 23: 857–861 - PubMed
-
- Bouwens L (2006) Beta cell regeneration. Curr Diabetes Rev 2: 3–9 - PubMed
-
- Lipsett M, Aikin R, Hanley S, Al-Maleek J, Laganiere S, Rosenburg L (2006) Islet neogenesis: a potential therapeutic tool in type 1 diabetes. Int J Biochem Cell Biol 38: 715–720 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
