

Trends in bilateral total knee arthroplasties: 153,259 discharges between 1990 and 2004
- PMID: 19002540
- PMCID: PMC2674161
- DOI: 10.1007/s11999-008-0610-z
Trends in bilateral total knee arthroplasties: 153,259 discharges between 1990 and 2004
Abstract
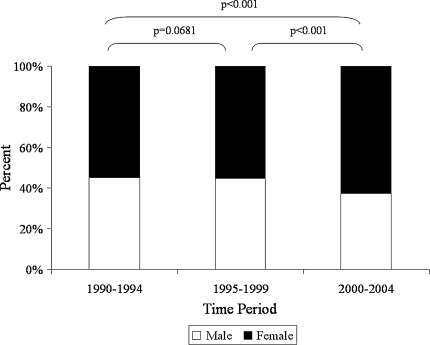
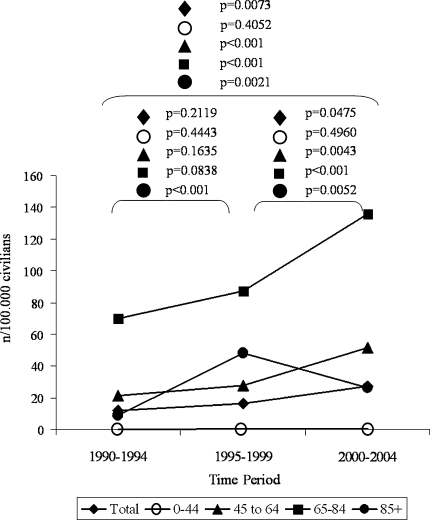
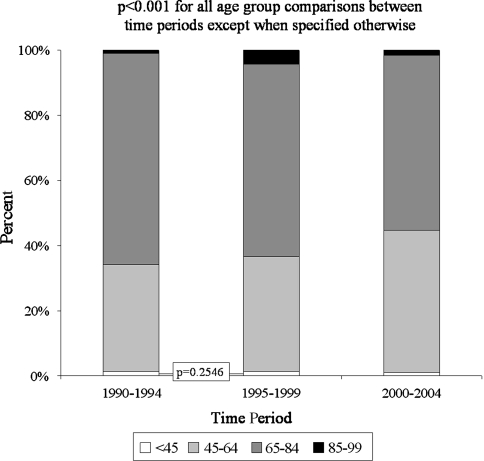
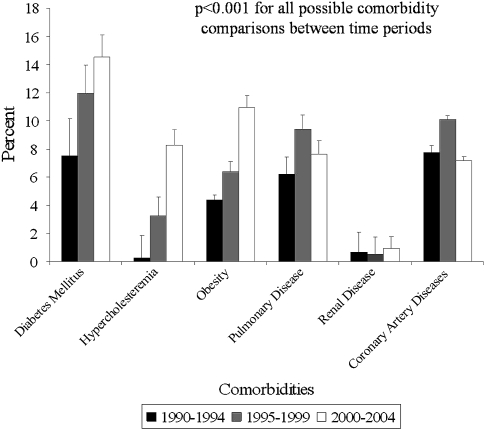
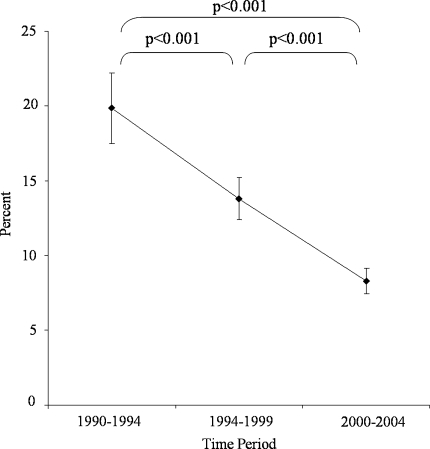
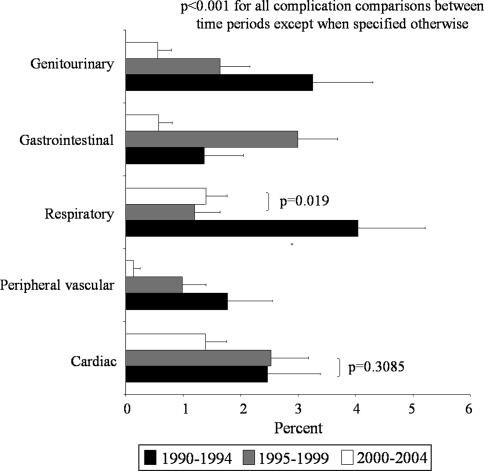
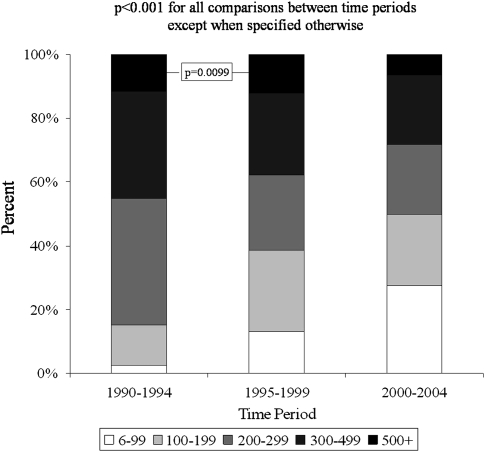
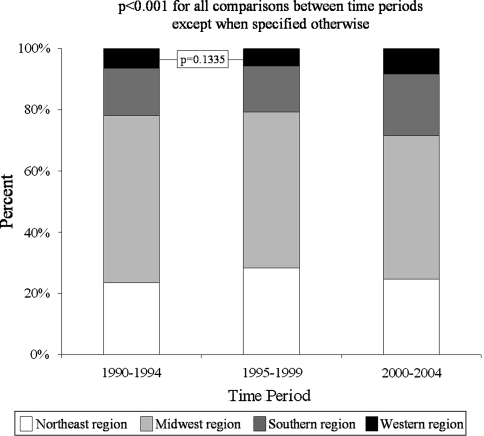
Information regarding national trends in bilateral TKAs is needed for a rational allocation of resources, policy making, and research. Therefore, we analyzed data from the National Hospital Discharge Survey to elucidate temporal changes in the demographics, comorbidity profiles, hospital stay, and in-hospital complications of patients undergoing bilateral TKAs in the United States. We created three 5-year periods: 1990-1994, 1995-1999, 2000-2004. Procedure, healthcare system, and patient-related variables were analyzed for an estimated 153,259 discharges. Use of bilateral TKAs more than doubled for the entire civilian population and almost tripled among the female population, with the steepest increase seen during the last two study periods. A decline of nearly 50% in the use of bilateral TKAs in patients 85 years and older was seen between the second and third study periods. The prevalence of coronary artery disease and pulmonary disease increased from the first to the second study periods but decreased from the second to the third. The changes in the variables studied may reflect a recently acquired reluctance to perform bilateral TKAs in elderly patients with cardiopulmonary comorbidities. Additional studies are necessary to identify other causal relationships and define the impact of these changes on various aspects of the healthcare system.
Level of evidence: Level II, prognostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures

References
-
- Bhattacharyya T, Iorio R, Healy WL. Rate of and risk factors for acute inpatient mortality after orthopaedic surgery. J Bone Joint Surg Am. 2002;84:562–572. - PubMed
-
- Design and Operation of the National Hospital Discharge Survey: 1988 Redesign. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 1988.
-
- Graves EJ. 1993 summary: National Hospital Discharge Survey. Adv Data. 1995;264:1–11. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
