

Fibromyalgia, systemic lupus erythematosus (SLE), and evaluation of SLE activity
- PMID: 19004039
- PMCID: PMC2944223
- DOI: 10.3899/jrheum.080212
Fibromyalgia, systemic lupus erythematosus (SLE), and evaluation of SLE activity
Abstract
Objective: To determine if fibromyalgia (FM) or fibromyalgia-ness (the tendency to respond to illness and psychosocial stress with fatigue, widespread pain, general increase in symptoms, and similar factors) is increased in patients with compared to those without systemic lupus erythematosus (SLE); to determine whether FM or fibromyalgia-ness biases the SLE Activity Questionnaire (SLAQ); and to determine if the SLAQ is overly sensitive to FM symptoms.
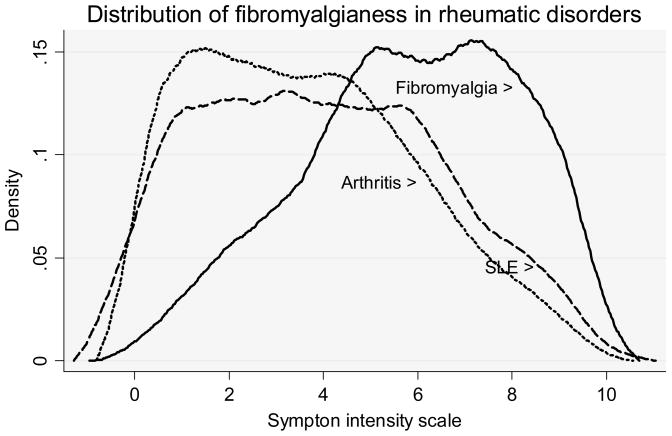
Methods: We developed a 16-item SLE Symptom Scale (SLESS) modeled on the SLAQ and used that scale to investigate the relation between SLE symptoms and fibromyalgia-ness in 23,321 patients with rheumatic disease. FM was diagnosed by survey FM criteria, and fibromyalgia-ness was measured using the Symptom Intensity (SI) Scale. As comparison groups, we combined patients with rheumatoid arthritis and noninflammatory rheumatic disorders into an "arthritis" group and also utilized a physician-diagnosed group of patients with FM.
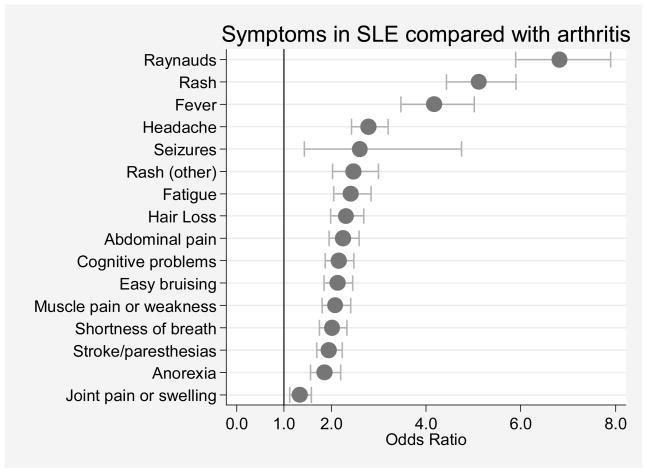
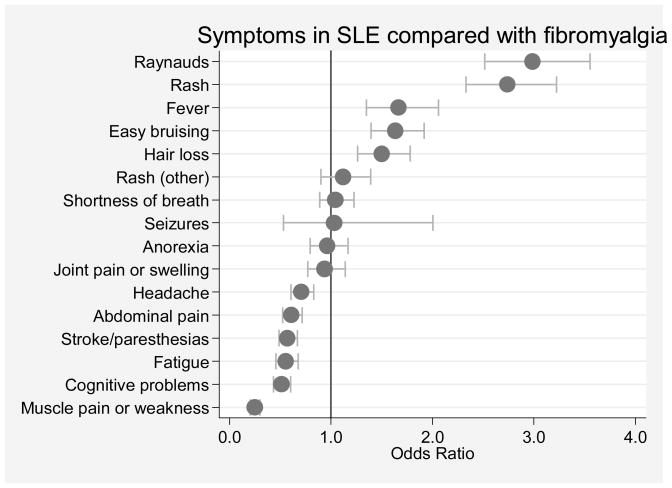
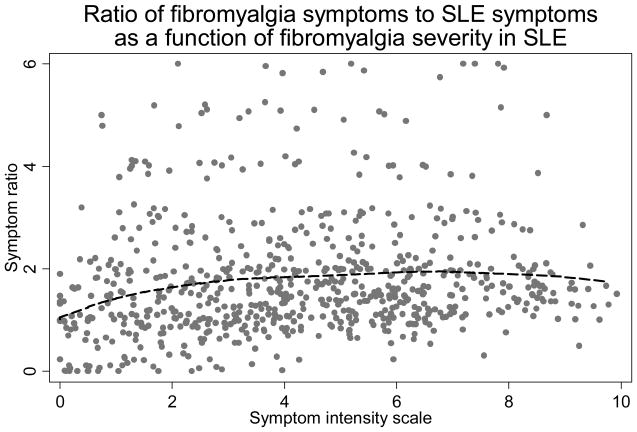
Results: FM was identified in 22.1% of SLE and 17.0% of those with arthritis. The SI scale was minimally increased in SLE. The correlation between SLAQ and SLESS was 0.738. SLESS/SLAQ scale items (Raynaud's phenomenon, rash, fever, easy bruising, hair loss) were significantly more associated with SLE than FM, while the reverse was true for headache, abdominal pain, paresthesias/stroke, fatigue, cognitive problems, and muscle pain or weakness. There was no evidence of disproportionate symptom-reporting associated with fibromyalgia-ness. Self-reported SLE was associated with an increased prevalence of FM that was unconfirmed by physicians, compared to SLE confirmed by physicians.
Conclusion: The prevalence of FM in SLE is minimally increased compared with its prevalence in patients with arthritis. Fibromyalgia-ness does not bias the SLESS and should not bias SLE assessments, including the SLAQ.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia.J Rheumatol. 2011 Jun;38(6):1113-22. doi: 10.3899/jrheum.100594. Epub 2011 Feb 1. J Rheumatol. 2011. PMID: 21285161
-
Using Clinical Characteristics and Patient-Reported Outcome Measures to Categorize Systemic Lupus Erythematosus Subtypes.Arthritis Care Res (Hoboken). 2021 Mar;73(3):386-393. doi: 10.1002/acr.24135. Arthritis Care Res (Hoboken). 2021. PMID: 31909888
-
Fatigue and widespread pain in systemic lupus erythematosus and Sjögren's syndrome: symptoms of the inflammatory disease or associated fibromyalgia?Clin Exp Rheumatol. 2012 Nov-Dec;30(6 Suppl 74):117-21. Epub 2012 Dec 14. Clin Exp Rheumatol. 2012. PMID: 23261010
-
Are patients with systemic lupus erythematosus at increased risk for fibromyalgia?Curr Rheumatol Rep. 2006 Dec;8(6):430-5. doi: 10.1007/s11926-006-0037-z. Curr Rheumatol Rep. 2006. PMID: 17092442 Review.
-
Pain and systemic lupus erythematosus.Reumatismo. 2014 Jun 6;66(1):33-8. doi: 10.4081/reumatismo.2014.762. Reumatismo. 2014. PMID: 24938194 Review.
Cited by
-
Measures of adult systemic lupus erythematosus: updated version of British Isles Lupus Assessment Group (BILAG 2004), European Consensus Lupus Activity Measurements (ECLAM), Systemic Lupus Activity Measure, Revised (SLAM-R), Systemic Lupus Activity Questionnaire for Population Studies (SLAQ), Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K), and Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI).Arthritis Care Res (Hoboken). 2011 Nov;63 Suppl 11(0 11):S37-46. doi: 10.1002/acr.20572. Arthritis Care Res (Hoboken). 2011. PMID: 22588757 Free PMC article. Review. No abstract available.
-
Comorbidity of Fibromyalgia in Primary Knee Osteoarthritis: Potential Impact on Functional Status and Quality of Life.Open Access Rheumatol. 2020 May 5;12:55-63. doi: 10.2147/OARRR.S252748. eCollection 2020. Open Access Rheumatol. 2020. PMID: 32440236 Free PMC article.
-
Real-world comparison of health care utilization between duloxetine and pregabalin initiators with fibromyalgia.J Pain Res. 2014 Jan 9;7:37-46. doi: 10.2147/JPR.S51636. eCollection 2014. J Pain Res. 2014. PMID: 24470771 Free PMC article.
-
Reliability, Feasibility, and Patient Acceptance of an Electronic Version of a Multidimensional Health Assessment Questionnaire for Routine Rheumatology Care: Validation and Patient Preference Study.JMIR Form Res. 2020 May 27;4(5):e15815. doi: 10.2196/15815. JMIR Form Res. 2020. PMID: 32459182 Free PMC article.
-
The prevalence of fibromyalgia in other chronic pain conditions.Pain Res Treat. 2012;2012:584573. doi: 10.1155/2012/584573. Epub 2011 Nov 17. Pain Res Treat. 2012. PMID: 22191024 Free PMC article.
References
-
- Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982;25:1271. - PubMed
-
- Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40(9):1725. - PubMed
-
- Middleton GD, Mcfarlin JE, Lipsky PE. The prevalence and clinical impact of fibromyalgia in systemic lupus erythematosus. Arthritis Rheum. 1994;37(8):1181–8. - PubMed
-
- Gladman DD, Urowitz MB, Gough J, MacKinnon A. Fibromyalgia is a major contributor to quality of life in lupus. J Rheumatol. 1997;24(11):2145–8. - PubMed
-
- Akkasilpa S, Goldman D, Magder LS, Petri M. Number of fibromyalgia tender points is associated with health status in patients with systemic lupus erythematosus. J Rheumatol. 2005;32(1):48–50. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials