

Timing of onset of CKD-related metabolic complications
- PMID: 19005010
- PMCID: PMC2615728
- DOI: 10.1681/ASN.2008020159
Timing of onset of CKD-related metabolic complications
Abstract
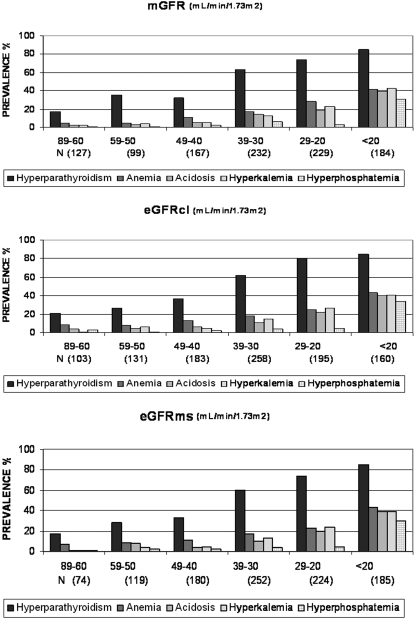
Chronic kidney disease (CKD) guidelines recommend evaluating patients with GFR <60 ml/min per 1.73 m(2) for complications, but little evidence supports the use of a single GFR threshold for all metabolic disorders. We used data from the NephroTest cohort, including 1038 adult patients who had stages 2 through 5 CKD and were not on dialysis, to study the occurrence of metabolic complications. GFR was measured using renal clearance of (51)Cr-EDTA (mGFR) and estimated using two equations derived from the Modification of Diet in Renal Disease study. As mGFR decreased from 60 to 90 to <20 ml/min per 1.73 m(2), the prevalence of hyperparathyroidism increased from 17 to 85%, anemia from 8 to 41%, hyperphosphatemia from 1 to 30%, metabolic acidosis from 2 to 39%, and hyperkalemia from 2 to 42%. Factors most strongly associated with metabolic complications, independent of mGFR, were younger age for acidosis and hyperphosphatemia, presence of diabetes for acidosis, diabetic kidney disease for anemia, and both male gender and the use of inhibitors of the renin-angiotensin system for hyperkalemia. mGFR thresholds for detecting complications with 90% sensitivity were 50, 44, 40, 39, and 37 ml/min per 1.73 m(2) for hyperparathyroidism, anemia, acidosis, hyperkalemia, and hyperphosphatemia, respectively. Analysis using estimated GFR produced similar results. In summary, this study describes the onset of CKD-related complications at different levels of GFR; anemia and hyperparathyroidism occur earlier than acidosis, hyperkalemia, and hyperphosphatemia.
Figures
References
-
- K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis 39: S1–S266, 2002 - PubMed
-
- Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, Hallan HA, Lydersen S, Holmen J: International comparison of the relationship of chronic kidney disease prevalence and ESRD risk. J Am Soc Nephrol 17: 2275–2284, 2006 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Bailey JL: Metabolic acidosis: An unrecognized cause of morbidity in the patient with chronic kidney disease. Kidney Int Suppl S15–S23, 2005 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
