

Review
doi: 10.1056/NEJMcp0804745.
Clinical practice. Anterior cruciate ligament tear
Affiliations
- PMID: 19005197
- PMCID: PMC3782299
- DOI: 10.1056/NEJMcp0804745
Item in Clipboard
Review
Clinical practice. Anterior cruciate ligament tear
N Engl J Med.
.
No abstract available
Figures
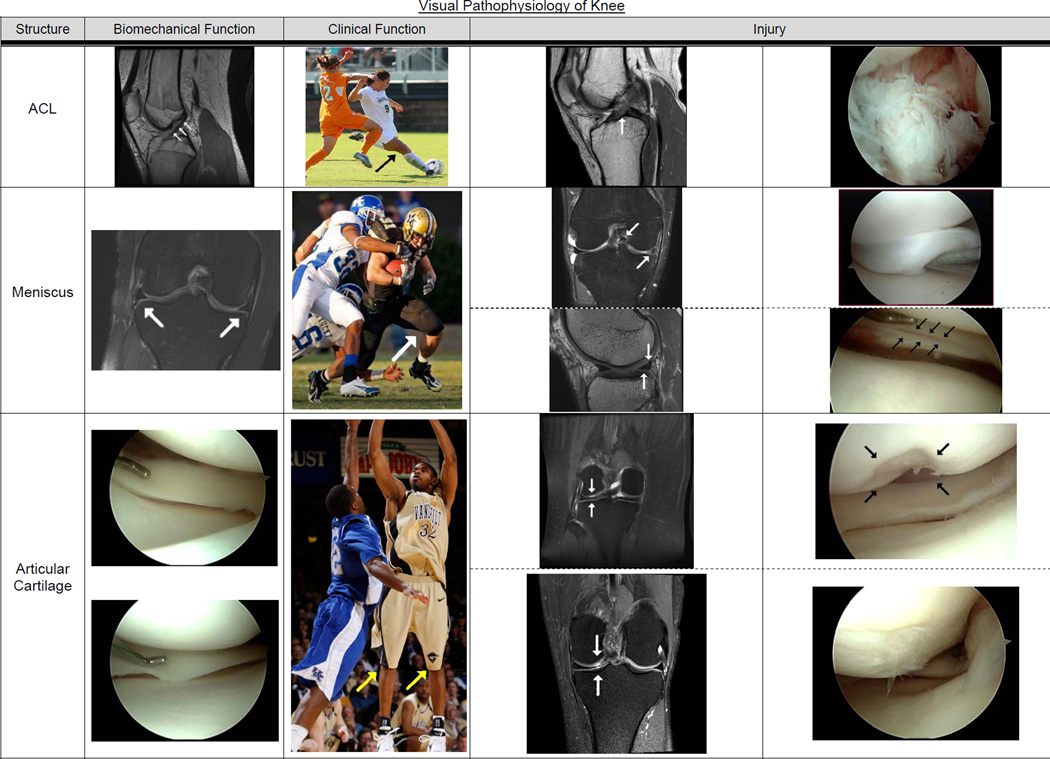
This figure contains MRIs, action photography, and operative pictures representing normal knees and tears to the ACL, meniscus, and articular cartilage. Row 1: Presents the ACL, shown from left to right. Arrows on the first MRI depict a normal ACL. Next is an action shot of a women’s soccer player planting her right leg to decelerate, pivot, and kick with her left leg. The second MRI shows the ACL tear as a disruption of the normal straight black contour of an ACL, and the operative picture indicates a completely torn ACL “balled up” in the front of the notch. Row 2: Meniscus -- The first MRI shows the medial and lateral menisci in the coronal plane (view from the front) as triangular black structures between femoral condyles above and tibial plateau below to distribute loads between meniscus and articular cartilage. The function of “load sharing” is depicted in the football running back with two players tackling him. Meniscus tears include a bucket handle tear shown above where a large portion is displaced into the notch (see arrow), which locks the knee (restricts motion). The corresponding operative picture (immediately to right) shows a large piece or bucket handle displaced blocking the normal view medial compartment. The lateral view by the arrow shows one of the most common acute tears of the meniscus as a white line straight through the posterior horn of the lateral meniscus. In the operative photograph the arrows indicate the tear. Row 3: The articular cartilage is a few-millimeter thick avascular covering over the femur and tibia (not unlike the rubber on a tire covering the steel belts). This surface is nearly frictionless by design to dissipate impact loads. The percentage of load between the meniscus versus the articular cartilage depends on which meniscus, degree of knee flexion, and integrity of the ACL. The basketball player demonstrates the ability of the articular cartilage to dissipate acute loads when landing from a jump. Articular cartilage pathology can be either focal defects as depicted on top or degenerative or arthritis as shown below. For the focal defect seen on MRI with corresponding intraoperative picture, there are current treatments available for restoring short-term function. However, once degenerative arthritis develops as shown by abnormal signal on an MRI and fibrillation shown intraop (contrast with the normally perfectly smooth articular surface), there are no effective treatments yet. The ACL tears can be reconstructed and meniscus tears either repaired or resected, enabling the athlete to return to play. The development of arthritis is the end of an athlete’s career regardless of age. Figure edited by Alex Bottiggi All athletic photographs courtesy of Rod Williamson, Vanderbilt Athletic Sports Information Director
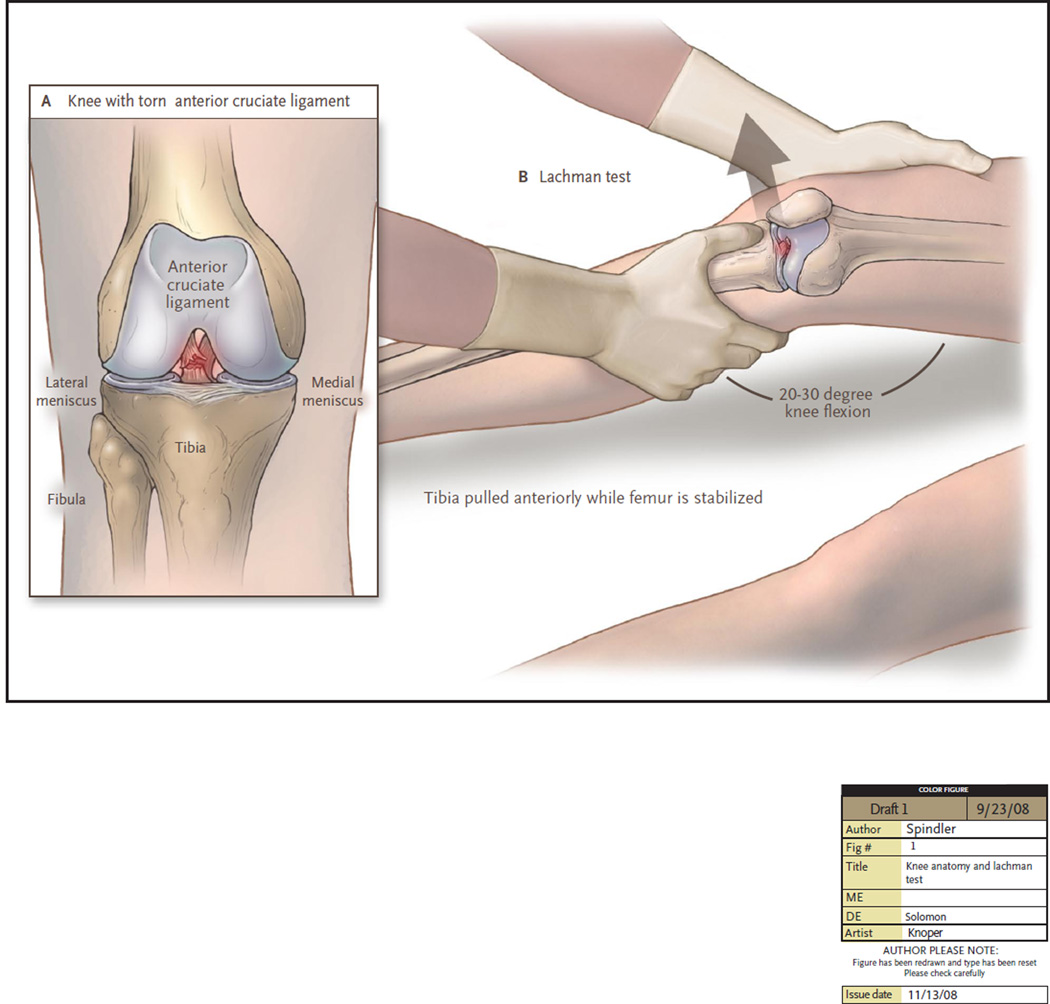
The most popular variation of “Lachman’s test” for ACL tears requires a supine relaxed patient. The examiner has one hand on the outside of the thigh, just above the knee, stabilizing the femur in slight external rotation and elevated off the bed to produce a knee flexion angle of 20–30 degrees. The second hand is placed on anteromedial tibia with thumb on flat bony border of tibia. Once the patient is relaxed the hand on the tibia attempts to displace the tibia anteriorly in relation to the stabilized femur. First the normal knee is examined as a control with a positive test on the injured knee the absent sensation of a solid stop (“endpoint”) to anterior displacement of tibia (called “soft endpoint”). Additional supporting information is an increased displacement of tibia anteriorly versus contralateral normal knee. The pivot shift has many variations but reproduces the subluxation of the tibia on the femur that the athlete feels clinically and is beyond the scope of this text.
Comment in
-
Anterior cruciate ligament tear.N Engl J Med. 2009 Apr 2;360(14):1463; author reply 1463. doi: 10.1056/NEJMc082471. N Engl J Med. 2009. PMID: 19339730 No abstract available.
References
-
- Gottlob CA, Baker CL, Jr, Pellissier JM, Colvin L. Cost effectiveness of anterior cruciate ligament reconstruction in young adults. Clin Orthop Relat Res. 1999:272–282. - PubMed
-
- Mountcastle SB, Posner M, Kragh JF, Jr, Taylor DC. Gender differences in anterior cruciate ligament injury vary with activity: epidemiology of anterior cruciate ligament injuries in a young, athletic population. Am J Sports Med. 2007;35:1635–1642. - PubMed
-
- Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35:1756–1769. - PubMed
-
- Agel J, Arendt EA, Bershadsky B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: a 13-year review. Am J Sports Med. 2005;33:524–531. - PubMed
-
- Bjordal JM, Arnoy F, Hannestad B, Strand T. Epidemiology of anterior cruciate ligament injuries in soccer. Am J Sports Med. 1997;25:341–345. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical