

Does short-term virologic failure translate to clinical events in antiretroviral-naïve patients initiating antiretroviral therapy in clinical practice?
- PMID: 19005271
- PMCID: PMC2793403
- DOI: 10.1097/QAD.0b013e328318f130
Does short-term virologic failure translate to clinical events in antiretroviral-naïve patients initiating antiretroviral therapy in clinical practice?
Abstract
Objective: To determine whether differences in short-term virologic failure among commonly used antiretroviral therapy (ART) regimens translate to differences in clinical events in antiretroviral-naïve patients initiating ART.
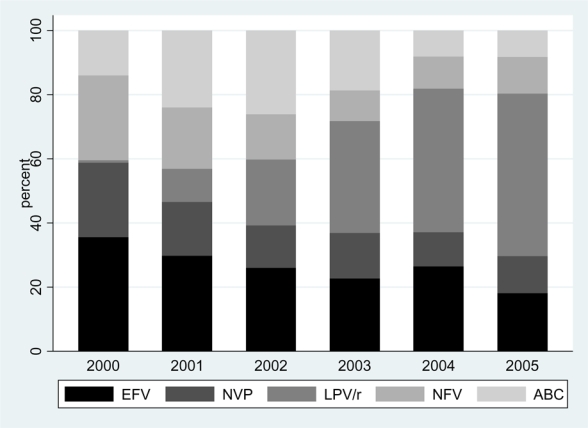
Design: Observational cohort study of patients initiating ART between January 2000 and December 2005.
Setting: The Antiretroviral Therapy Cohort Collaboration (ART-CC) is a collaboration of 15 HIV cohort studies from Canada, Europe, and the United States.
Study participants: A total of 13 546 antiretroviral-naïve HIV-positive patients initiating ART with efavirenz, nevirapine, lopinavir/ritonavir, nelfinavir, or abacavir as third drugs in combination with a zidovudine and lamivudine nucleoside reverse transcriptase inhibitor backbone.
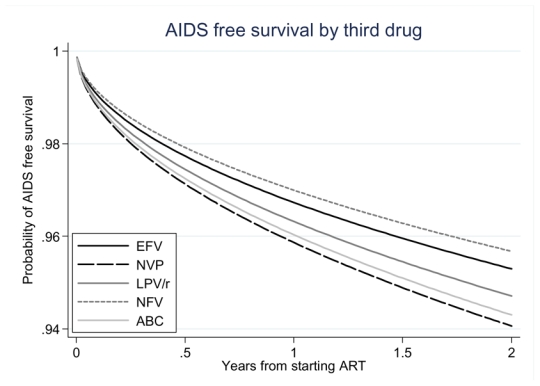
Main outcome measures: Short-term (24-week) virologic failure (>500 copies/ml) and clinical events within 2 years of ART initiation (incident AIDS-defining event, death, and a composite measure of these two outcomes).
Results: Compared with efavirenz as initial third drug, short-term virologic failure was more common with all other third drugs evaluated; nevirapine (adjusted odds ratio = 1.87, 95% confidence interval (CI) = 1.58-2.22), lopinavir/ritonavir (1.32, 95% CI = 1.12-1.57), nelfinavir (3.20, 95% CI = 2.74-3.74), and abacavir (2.13, 95% CI = 1.82-2.50). However, the rate of clinical events within 2 years of ART initiation appeared higher only with nevirapine (adjusted hazard ratio for composite outcome measure 1.27, 95% CI = 1.04-1.56) and abacavir (1.22, 95% CI = 1.00-1.48).
Conclusion: Among antiretroviral-naïve patients initiating therapy, between-ART regimen, differences in short-term virologic failure do not necessarily translate to differences in clinical outcomes. Our results should be interpreted with caution because of the possibility of residual confounding by indication.
Figures
References
-
- Palella FJ, Jr, Baker RK, Moorman AC, Chmiel JS, Wood KC, Brooks JT, Holmberg SD. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. - PubMed
-
- Sabin CA, Smith CJ, Youle M, Lampe FC, Bell DR, Puradiredja D, et al. Deaths in the era of HAART: contribution of late presentation, treatment exposure, resistance and abnormal laboratory markers. Aids. 2006;20:67–71. - PubMed
-
- van Sighem AI, van de Wiel MA, Ghani AC, Jambroes M, Reiss P, Gyssens IC, et al. Mortality and progression to AIDS after starting highly active antiretroviral therapy. Aids. 2003;17:2227–2236. - PubMed
-
- Hughes MD. Initial treatment of HIV infection: randomized trials with clinical end points are still needed. J Infect Dis. 2006;194:542–544. - PubMed
-
- Walker AM. Confounding by indication. Epidemiology. 1996;7:335–336. - PubMed
