

Incidence of bullosis diabeticorum--a controversial cause of chronic foot ulceration
- PMID: 19006577
- PMCID: PMC7951251
- DOI: 10.1111/j.1742-481X.2008.00476.x
Incidence of bullosis diabeticorum--a controversial cause of chronic foot ulceration
Abstract
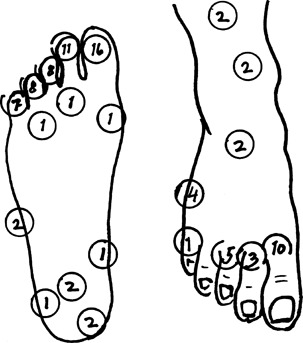
Bullosis diabeticorum (BD) is considered a rare and relatively harmless skin manifestation with tense blisters appearing rapidly and mostly on the feet. Most papers report only a few cases and the cause of the blisters is not known. We have experienced that the lesions are not so rare and may turn into chronic foot ulcers with complications. Retrospective study of 25 consecutive patients with 35 outbreaks and 93 bullae in a population of 5000 people with diabetes treated during a 3-year period. The bullae were deroofed in order to examine the bulla base and treated as foot ulcers including debridement, antibiotics, bandage and protective footwear. The incidence of BD per year in the present diabetic population is 0.16%. In 29 outbreaks, there were hypoglycaemic episodes or highly varying blood glucose. Antibiotics were given in 17 of 35 episodes. Time to healing was as much as median 2.5 months (range 0.5-23 months). Two patients had minor amputations. BD should be well known to all members of diabetic foot care teams. Blood glucose control with special attention to hypoglycaemia at the time of eruption, deroofing of the bullae and foot ulcer care are recommended.
Figures






Similar articles
-
[Bullosis diabeticorum : Two case studies].Hautarzt. 2018 Sep;69(9):751-755. doi: 10.1007/s00105-018-4132-7. Hautarzt. 2018. PMID: 29468278 German.
-
Bullosis diabeticorum. A report of two cases with a review of the literature.J Am Podiatr Med Assoc. 1991 Oct;81(10):561-3. doi: 10.7547/87507315-81-10-561. J Am Podiatr Med Assoc. 1991. PMID: 1774644
-
[Bullosis diabeticorum: report of ten cases].Tunis Med. 2009 Nov;87(11):747-9. Tunis Med. 2009. PMID: 20209832 French.
-
Bullosis diabeticorum: case report and review.N Z Med J. 2013 Mar 15;126(1371):91-4. N Z Med J. 2013. PMID: 23793125 Review.
-
Diabetic bullae: a case series and a new model of surgical management.J Wound Care. 2014 Jun;23(6):326, 328-30. doi: 10.12968/jowc.2014.23.6.326. J Wound Care. 2014. PMID: 24920203 Review.
Cited by
-
Efficacy and long-term longitudinal follow-up of bone marrow mesenchymal cell transplantation therapy in a diabetic patient with recurrent lower limb bullosis diabeticorum.Stem Cell Res Ther. 2018 Apr 10;9(1):99. doi: 10.1186/s13287-018-0854-9. Stem Cell Res Ther. 2018. PMID: 29631615 Free PMC article. Clinical Trial.
-
Bullosis diabeticorum in a morbidly obese woman in Haiti.Arch Clin Cases. 2023 Dec 28;10(4):196-199. doi: 10.22551/2023.41.1004.10274. eCollection 2023. Arch Clin Cases. 2023. PMID: 38155997 Free PMC article.
-
Bullosis Diabeticorum: A Rare Presentation with Immunoglobulin G (IgG) Deposition Related Vasculopathy. Case Report and Focused Review.Am J Case Rep. 2018 Jan 15;19:52-56. doi: 10.12659/ajcr.905452. Am J Case Rep. 2018. PMID: 29332930 Free PMC article. Review.
-
Bullosis diabeticorum: rare presentation in a common disease.Case Rep Endocrinol. 2014;2014:862912. doi: 10.1155/2014/862912. Epub 2014 Nov 18. Case Rep Endocrinol. 2014. PMID: 25478251 Free PMC article.
-
[Bullosis diabeticorum : Two case studies].Hautarzt. 2018 Sep;69(9):751-755. doi: 10.1007/s00105-018-4132-7. Hautarzt. 2018. PMID: 29468278 German.
References
-
- Bernstein JE, Medenica M, Soltani K, Griem SF. Bullous eruption of diabetes mellitus. Arch Dermatol 1979;115:324–5. - PubMed
-
- Basarab T, Munn SE, McGrath J, Russell JR. Bullosis diabeticorum. A case report and literature review. Clin Exp Dermatol 1995;20:218–20. - PubMed
-
- Borner C, Herzog E, Hild R, Hopker WW. [Bullosis diabeticorum: 2 follow‐up studies]. Med Klin (Munich) 1987;82:165–8. - PubMed
-
- Cantwell AR Jr, Martz W. Idiopathic bullae in diabetics. Bullosis diabeticorum. Arch Dermatol 1967;96:42–4. - PubMed
-
- Cope RL. Spontaneous bulla formation in the skin in diabetes mellitus. Ann Intern Med 1950;32:964–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
