

Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis
- PMID: 19008265
- PMCID: PMC2583392
- DOI: 10.1136/bmj.a2313
Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis
Erratum in
- BMJ.2009;338:b1881
Abstract
Objective: To determine the effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome.
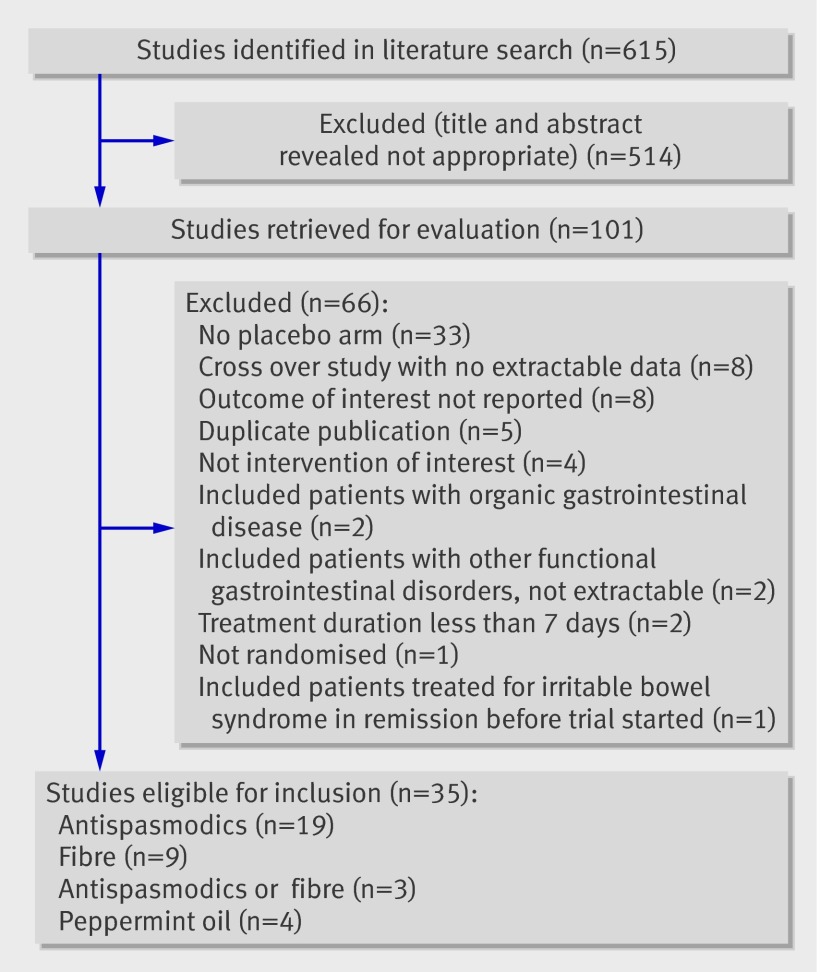
Design: Systematic review and meta-analysis of randomised controlled trials.
Data sources: Medline, Embase, and the Cochrane controlled trials register up to April 2008. Review methods Randomised controlled trials comparing fibre, antispasmodics, and peppermint oil with placebo or no treatment in adults with irritable bowel syndrome were eligible for inclusion. The minimum duration of therapy considered was one week, and studies had to report either a global assessment of cure or improvement in symptoms, or cure of or improvement in abdominal pain, after treatment. A random effects model was used to pool data on symptoms, and the effect of therapy compared with placebo or no treatment was reported as the relative risk (95% confidence interval) of symptoms persisting.
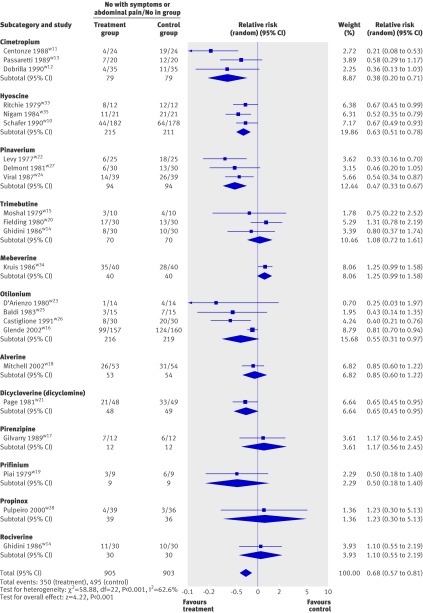
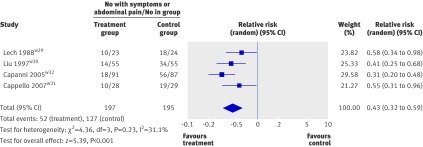
Results: 12 studies compared fibre with placebo or no treatment in 591 patients (relative risk of persistent symptoms 0.87, 95% confidence interval 0.76 to 1.00). This effect was limited to ispaghula (0.78, 0.63 to 0.96). Twenty two trials compared antispasmodics with placebo in 1778 patients (0.68, 0.57 to 0.81). Various antispasmodics were studied, but otilonium (four trials, 435 patients, relative risk of persistent symptoms 0.55, 0.31 to 0.97) and hyoscine (three trials, 426 patients, 0.63, 0.51 to 0.78) showed consistent evidence of efficacy. Four trials compared peppermint oil with placebo in 392 patients (0.43, 0.32 to 0.59).
Conclusion: Fibre, antispasmodics, and peppermint oil were all more effective than placebo in the treatment of irritable bowel syndrome.
Conflict of interest statement
Competing interests: NJT has received consultancy fees from Procter and Gamble, Lexicon Genetics, Astellas Pharma US, Pharma Frontiers, Callisto Pharmaceuticals, AstraZeneca, Addex Pharma, Ferring Pharma, Salix, MGI Pharma, McNeil Consumer, Microbia, Dynogen, Conexus, Novartis, and Metabolic Pharmaceuticals, and has received research support from Novartis, Takeda, GlaxoSmithKline, Dynogen, and Tioga. EMMQ has received consultant’s and speaker’s bureau fees from Nycomed, Boehringer Ingelheim, Procter and Gamble, Reckitt Benckiser, and Prometheus, and holds equity in Alimentary Health. PM holds a chair at McMaster University partly funded by an unrestricted donation by AstraZeneca, and has received consultant’s and speaker’s bureau fees from AstraZeneca, AxCan Pharma, Nycomed, and Johnson and Johnson.
Figures

Comment in
-
Irritable bowel syndrome. Why pills more than skills?BMJ. 2009 Jan 6;338:a3148. doi: 10.1136/bmj.a3148. BMJ. 2009. PMID: 19126613 No abstract available.
-
The problem of insoluble fibre in irritable bowel syndrome.BMJ. 2009 Jan 6;338:a3149. doi: 10.1136/bmj.a3149. BMJ. 2009. PMID: 19126614 No abstract available.
-
Review: fibre, antispasmodics, and peppermint oil are all effective for irritable bowel syndrome.Evid Based Med. 2009 Jun;14(3):84. doi: 10.1136/ebm.14.3.84. Evid Based Med. 2009. PMID: 19483033 No abstract available.
References
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology 2006;130:1480-91. - PubMed
-
- Agreus L, Talley NJ, Svardsudd K, Tibblin G, Jones MP. Identifying dyspepsia and irritable bowel syndrome: the value of pain or discomfort, and bowel habit descriptors. Scand J Gastroenterol 2000;35:142-51. - PubMed
-
- Hillila MT, Farkkila MA. Prevalence of irritable bowel syndrome according to different diagnostic criteria in a non-selected adult population. Aliment Pharmacol Ther 2004;20:339-45. - PubMed
-
- Hungin APS, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: an international survey of 40 000 subjects. Aliment Pharmacol Ther 2003;17:643-50. - PubMed
-
- McKee DP, Quigley EM. Intestinal motility in irritable bowel syndrome: Is IBS a motility disorder? Part 1. Definition of IBS and colonic motility. Dig Dis Sci 1993;38:1761-2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous