

Ankle: isotropic MR imaging with 3D-FSE-cube--initial experience in healthy volunteers
- PMID: 19011194
- PMCID: PMC2691812
- DOI: 10.1148/radiol.2493080227
Ankle: isotropic MR imaging with 3D-FSE-cube--initial experience in healthy volunteers
Abstract
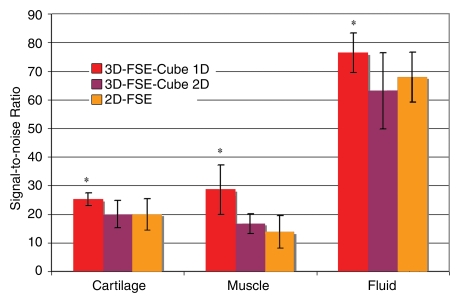
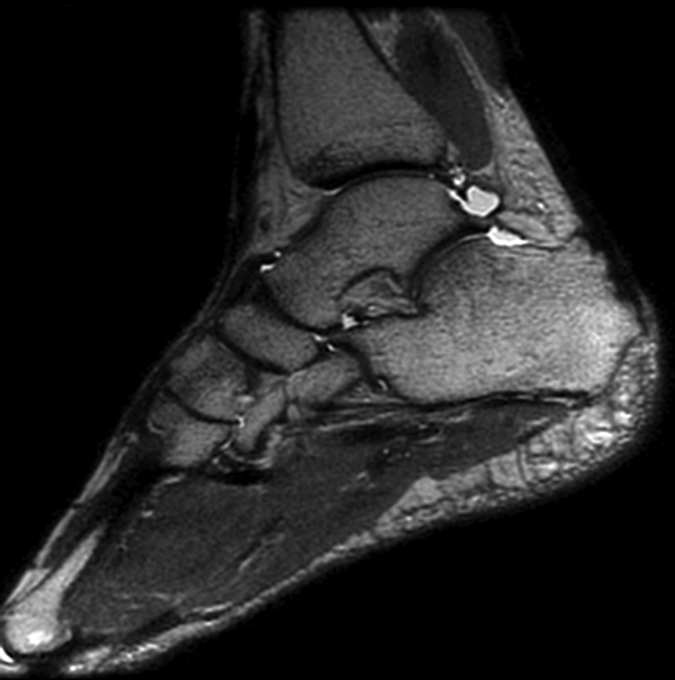
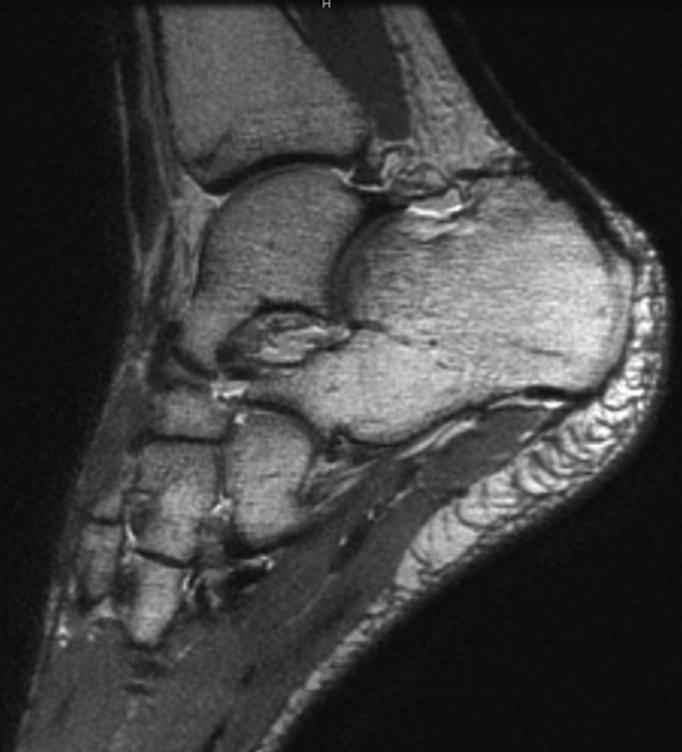
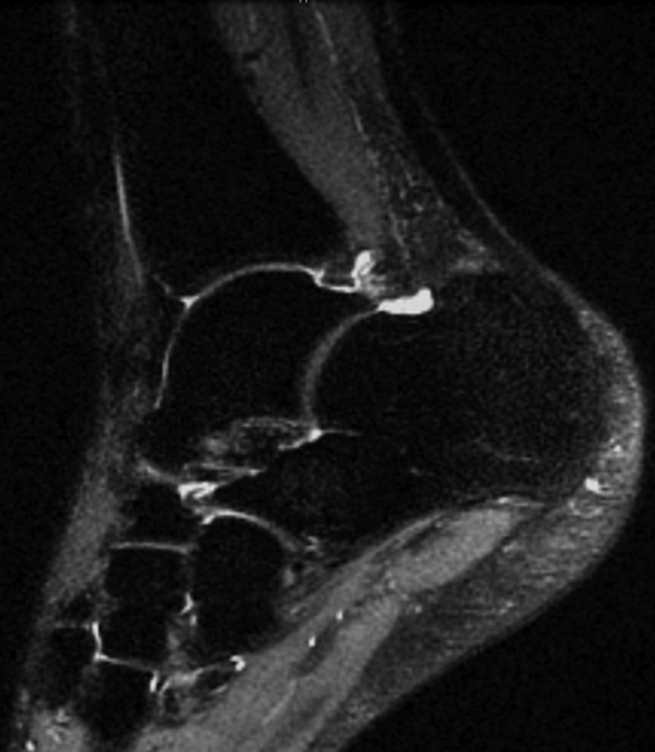
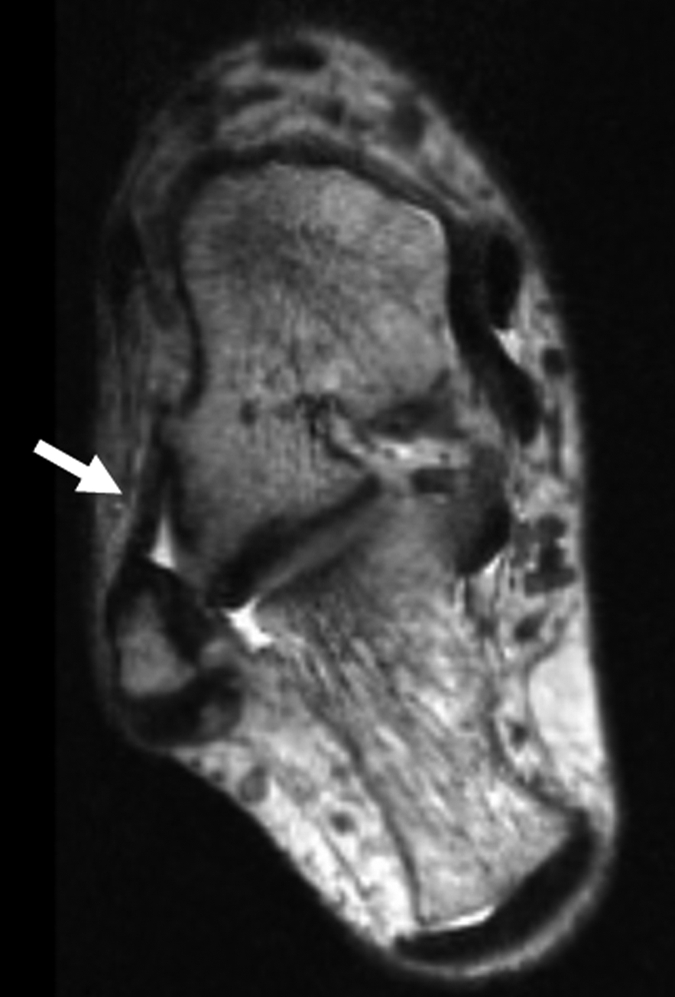
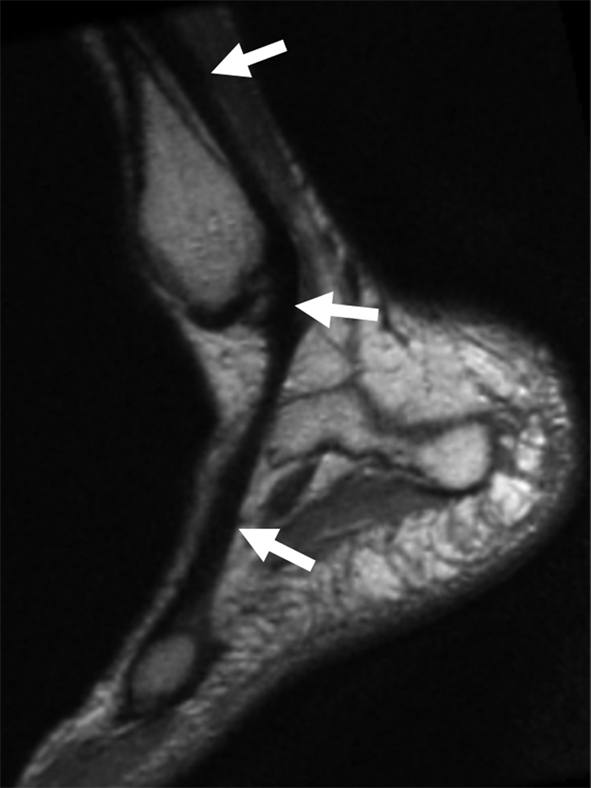
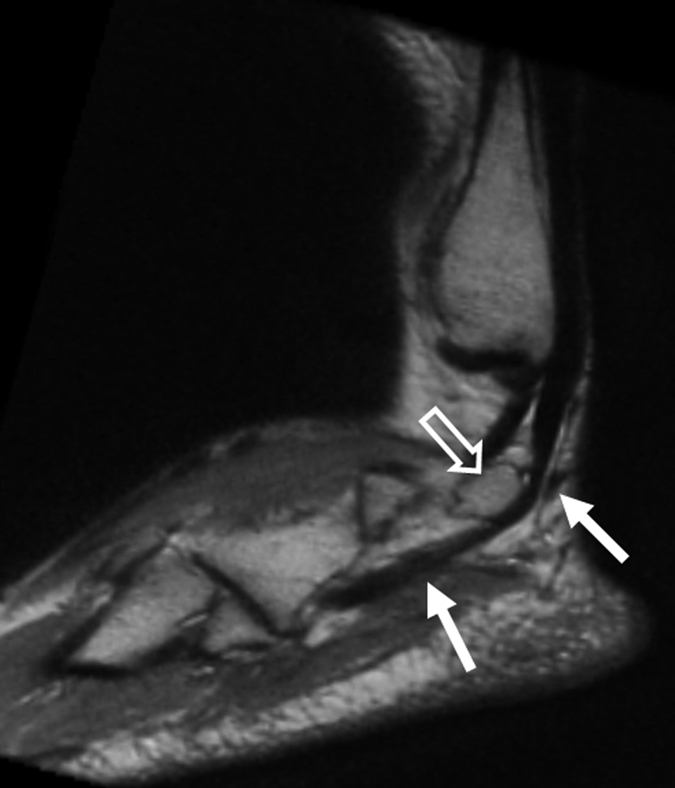
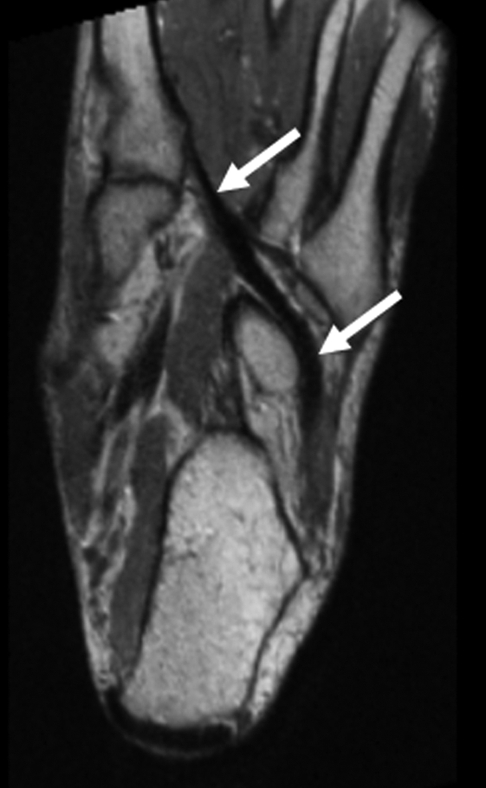
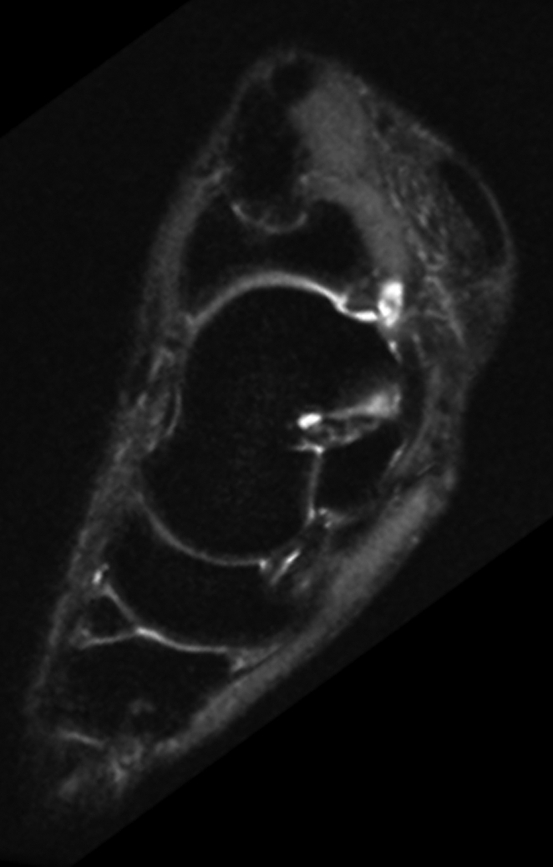
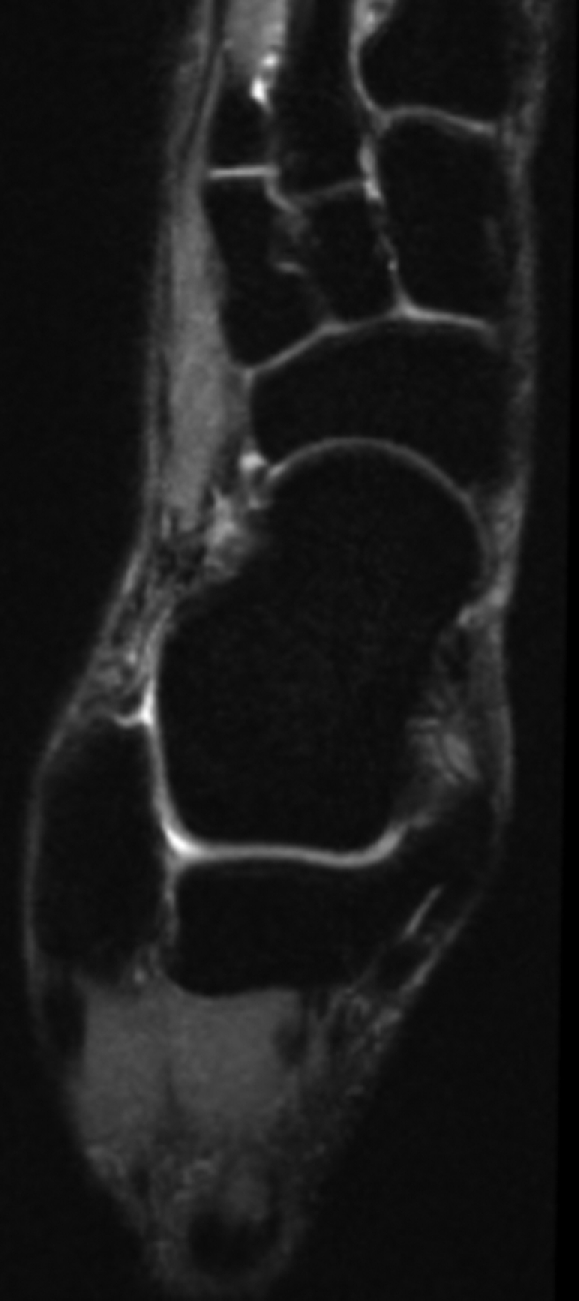
The purpose of this prospective study was to compare a new isotropic three-dimensional (3D) fast spin-echo (FSE) pulse sequence with parallel imaging and extended echo train acquisition (3D-FSE-Cube) with a conventional two-dimensional (2D) FSE sequence for magnetic resonance (MR) imaging of the ankle. After institutional review board approval and informed consent were obtained and in accordance with HIPAA privacy guidelines, MR imaging was performed in the ankles of 10 healthy volunteers (four men, six women; age range, 25-41 years). Imaging with the 3D-FSE-Cube sequence was performed at 3.0 T by using both one-dimensional- and 2D-accelerated autocalibrated parallel imaging to decrease imaging time. Signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR) with 3D-FSE-Cube were compared with those of the standard 2D FSE sequence. Cartilage, muscle, and fluid SNRs were significantly higher with the 3D-FSE-Cube sequence (P < .01 for all). Fluid-cartilage CNR was similar for both techniques. The two sequences were also compared for overall image quality, blurring, and artifacts. No significant difference for overall image quality and artifacts was demonstrated between the 2D FSE and 3D-FSE-Cube sequences, although the section thickness in 3D-FSE-Cube imaging was much thinner (0.6 mm). However, blurring was significantly greater on the 3D-FSE-Cube images (P < .04). The 3D-FSE-Cube sequence with isotropic resolution is a promising new MR imaging sequence for viewing complex joint anatomy.
RSNA, 2008
Figures





Similar articles
-
Imaging of the wrist at 1.5 Tesla using isotropic three-dimensional fast spin echo cube.J Magn Reson Imaging. 2011 Apr;33(4):908-15. doi: 10.1002/jmri.22494. J Magn Reson Imaging. 2011. PMID: 21448957 Free PMC article.
-
Isotropic MRI of the knee with 3D fast spin-echo extended echo-train acquisition (XETA): initial experience.AJR Am J Roentgenol. 2007 May;188(5):1287-93. doi: 10.2214/AJR.06.1208. AJR Am J Roentgenol. 2007. PMID: 17449772
-
[Three-dimensional isotropic magnetic resonance imaging of the ankle joint].Nan Fang Yi Ke Da Xue Xue Bao. 2015 Jun;35(6):862-7. Nan Fang Yi Ke Da Xue Xue Bao. 2015. PMID: 26111686 Chinese.
-
3D MRI of the Ankle: A Concise State-of-the-Art Review.Semin Musculoskelet Radiol. 2021 Jun;25(3):514-526. doi: 10.1055/s-0041-1731332. Epub 2021 Sep 21. Semin Musculoskelet Radiol. 2021. PMID: 34547816 Review.
-
3D isotropic MRI of ankle: review of literature with comparison to 2D MRI.Skeletal Radiol. 2024 May;53(5):825-846. doi: 10.1007/s00256-023-04513-2. Epub 2023 Nov 18. Skeletal Radiol. 2024. PMID: 37978990 Review.
Cited by
-
Qualitative and quantitative assessment of isotropic ankle magnetic resonance imaging: three-dimensional isotropic intermediate-weighted turbo spin echo versus three-dimensional isotropic fast field echo sequences.Korean J Radiol. 2012 Jul-Aug;13(4):443-9. doi: 10.3348/kjr.2012.13.4.443. Epub 2012 Jun 18. Korean J Radiol. 2012. PMID: 22778566 Free PMC article.
-
[Advanced cartilage imaging for detection of cartilage injuries and osteochondral lesions].Radiologe. 2018 May;58(5):422-432. doi: 10.1007/s00117-017-0348-2. Radiologe. 2018. PMID: 29374314 Review. German.
-
Comparison of oblique coronal images in knee of three-dimensional isotropic T2-weighted turbo spin echo MRI versus two-dimensional fast spin echo T2-weighted sequences for evaluation of posterior cruciate ligament injury.Br J Radiol. 2016 Nov;89(1067):20160554. doi: 10.1259/bjr.20160554. Epub 2016 Sep 21. Br J Radiol. 2016. PMID: 27653673 Free PMC article.
-
Ligaments of the Lisfranc joint in MRI: 3D-SPACE (sampling perfection with application optimized contrasts using different flip-angle evolution) sequence compared to three orthogonal proton-density fat-saturated (PD fs) sequences.Skeletal Radiol. 2013 Mar;42(3):399-409. doi: 10.1007/s00256-012-1491-5. Epub 2012 Aug 23. Skeletal Radiol. 2013. PMID: 22915209
-
Quality comparison between three-dimensional T2-weighted SPACE and two-dimensional T2-weighted turbo spin echo magnetic resonance images for the brachytherapy planning evaluation of prostate and periprostatic anatomy.Brachytherapy. 2020 Jul-Aug;19(4):484-490. doi: 10.1016/j.brachy.2020.04.001. Epub 2020 May 10. Brachytherapy. 2020. PMID: 32402544 Free PMC article.
References
-
- Fong DT, Hong Y, Chan LK, Yung PS, Chan KM. A systematic review on ankle injury and ankle sprain in sports. Sports Med 2007;37:73–94. - PubMed
-
- Kirby AB, Beall DP, Murphy MP, Ly JQ, Fish JR. Magnetic resonance imaging findings of chronic lateral ankle instability. Curr Probl Diagn Radiol 2005;34:196–203. - PubMed
-
- Cheung Y, Rosenberg ZS. MR imaging of ligamentous abnormalities of the ankle and foot. Magn Reson Imaging Clin N Am 2001;9:507–531, x. - PubMed
-
- Frey C, Bell J, Teresi L, Kerr R, Feder K. A comparison of MRI and clinical examination of acute lateral ankle sprains. Foot Ankle Int 1996;17:533–537. - PubMed
-
- Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revised classification. Foot Ankle Int 1999;20:789–793. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
