

HIV-associated nephropathy: clinical presentation, pathology, and epidemiology in the era of antiretroviral therapy
- PMID: 19013322
- PMCID: PMC2656916
- DOI: 10.1016/j.semnephrol.2008.08.005
HIV-associated nephropathy: clinical presentation, pathology, and epidemiology in the era of antiretroviral therapy
Abstract
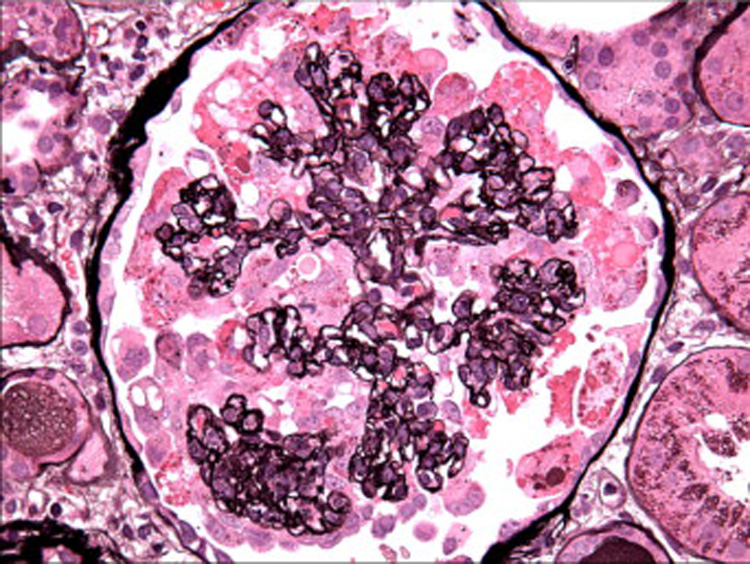
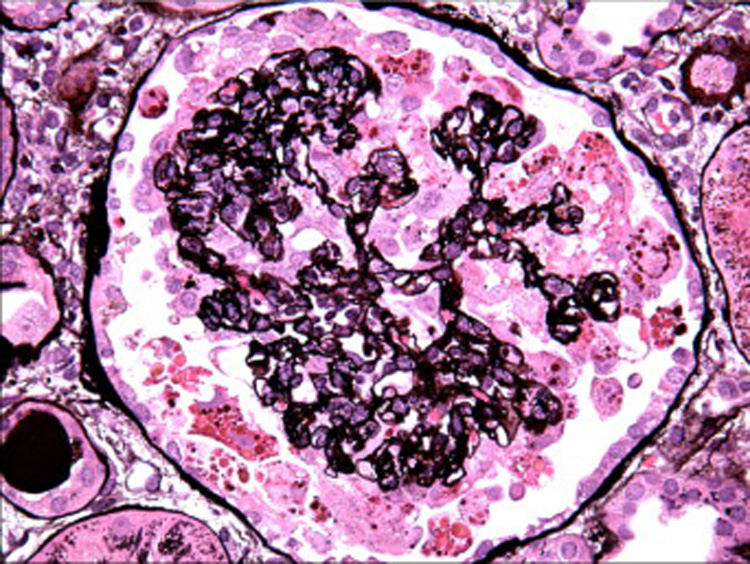
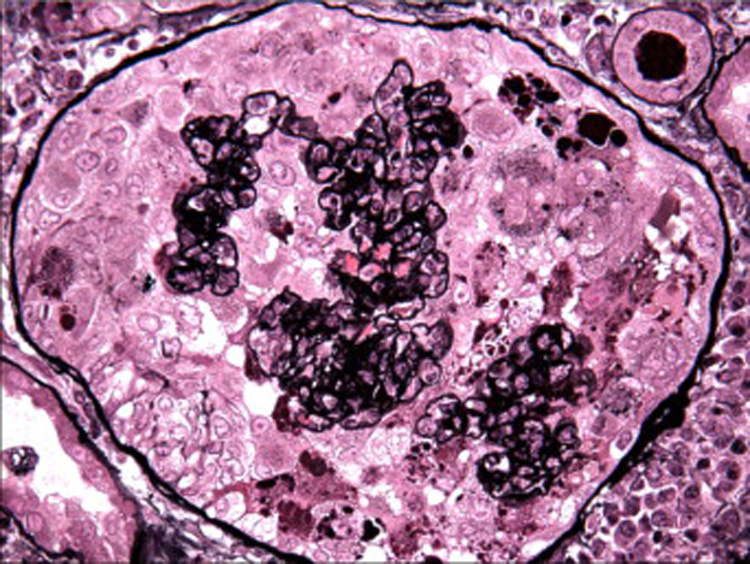
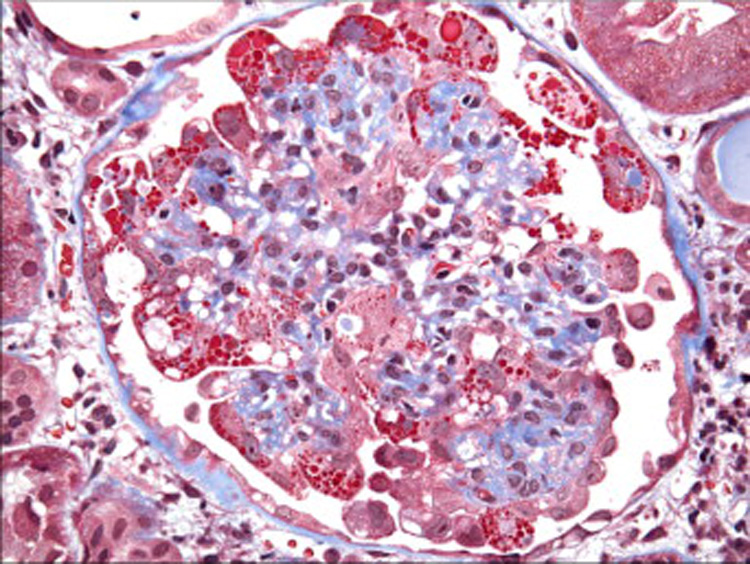
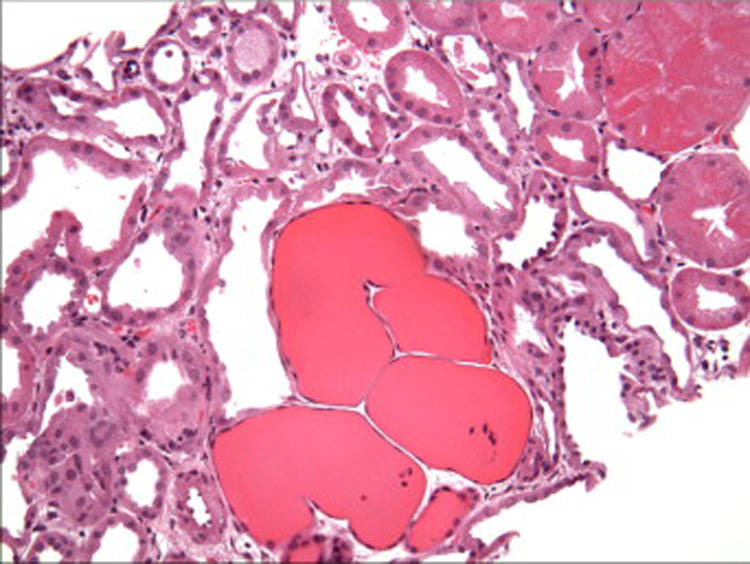
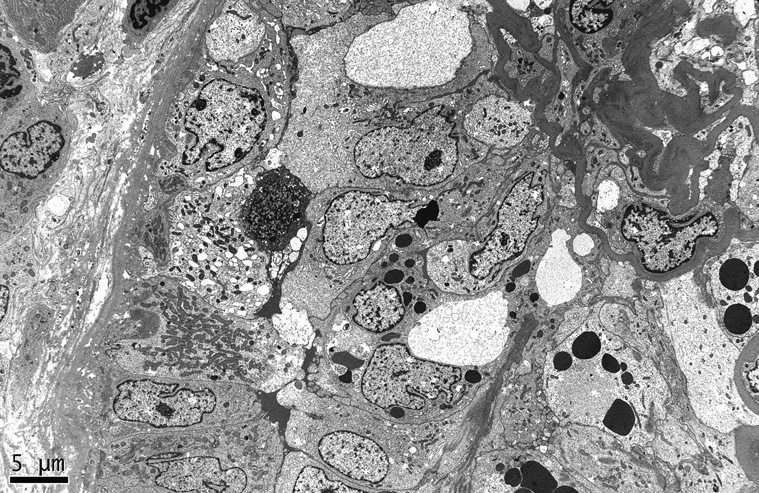
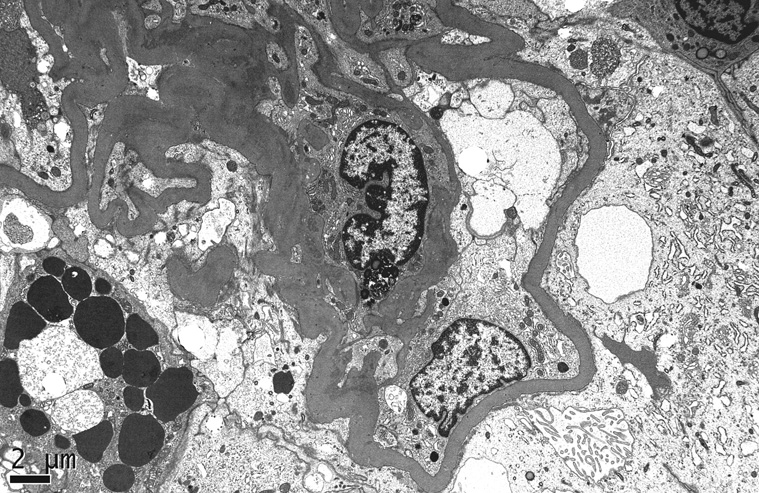
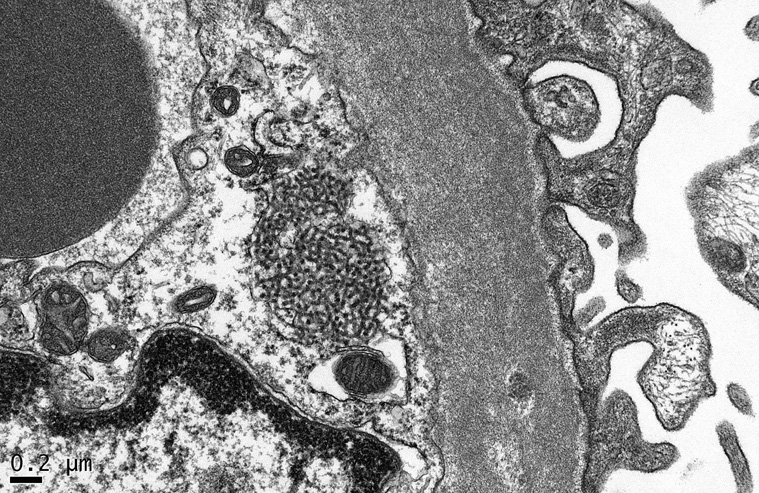
The classic kidney disease of human immunodeficiency virus (HIV) infection, HIV-associated nephropathy, is characterized by progressive acute renal failure, often accompanied by proteinuria and ultrasound findings of enlarged, echogenic kidneys. Definitive diagnosis requires kidney biopsy, which shows collapsing focal segmental glomerulosclerosis with associated microcystic tubular dilatation and interstitial inflammation. Podocyte proliferation is a hallmark of HIV-associated nephropathy, although this classic pathology is observed less frequently in antiretroviral-treated patients. The pathogenesis of HIV-associated nephropathy involves direct HIV infection of renal epithelial cells, and the widespread introduction of combination antiretroviral therapy has had a significant impact on the natural history and epidemiology of this unique disease. These observations have established antiretroviral therapy as the cornerstone of treatment for HIV-associated nephropathy in the absence of prospective clinical trials. Adjunctive therapy for HIV-associated nephropathy includes angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers, as well as corticosteroids in selected patients with significant interstitial inflammation or rapid progression.
Figures
References
-
- Rao TK, Filippone EJ, Nicastri AD, Landesman SH, Frank E, Chen CK, Friedman EA. Associated focal and segmental glomerulosclerosis in the acquired immunodeficiency syndrome. N Engl J Med. 1984;310:669–673. - PubMed
-
- Pardo V, Aldana M, Colton RM, Fischl MA, Jaffe D, Moskowitz L, Hensley GT, Bourgoignie JJ. Glomerular lesions in the acquired immunodeficiency syndrome. Ann Intern Med. 1984;101:429–434. - PubMed
-
- Gardenswartz MH, Lerner CW, Seligson GR, Zabetakis PM, Rotterdam H, Tapper ML, Michelis MF, Bruno MS. Renal disease in patients with AIDS: a clinicopathologic study. Clin Nephrol. 1984;21:197–204. - PubMed
-
- Ross MJ, Klotman PE. Recent progress in HIV-associated nephropathy. J Am Soc Nephrol. 2002;13:2997–3004. - PubMed
-
- U.S. Renal Data System. USRDS 2007 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. 2007.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
