

Review
doi: 10.1016/j.semnephrol.2008.09.001.
Kidney disease in HIV-positive children
Affiliations
- PMID: 19013330
- PMCID: PMC2778302
- DOI: 10.1016/j.semnephrol.2008.09.001
Item in Clipboard
Review
Kidney disease in HIV-positive children
Semin Nephrol.
2008 Nov.
Abstract
Before the era of highly active antiretroviral therapy, more than 40% of human immunodeficiency virus (HIV)-infected children experienced renal complications. In sub-Saharan Africa, approximately 2.1 million children are infected with HIV-1. In the absence of antiretroviral therapy, young African children frequently died of AIDS-related complications before renal diseases could be manifested or diagnosed. As antiretroviral therapy has become more available, and their survival has increased, our experience in treating kidney disease in HIV-infected children has improved. This article discusses relevant clinical and pathologic findings related to kidney disease in HIV-infected children.
Figures
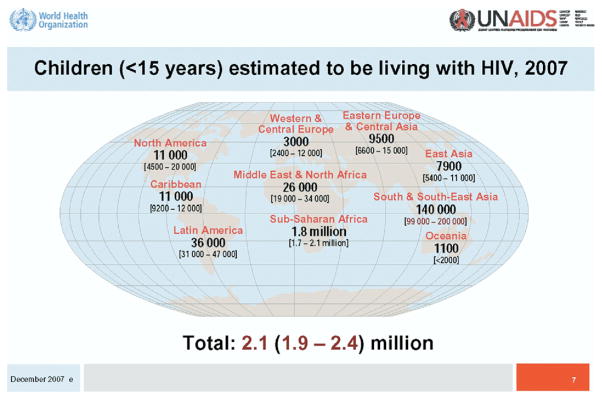
World Health Organization assessment of the number of children infected with HIV-1. Figure reprinted with permission from UNAIDS.
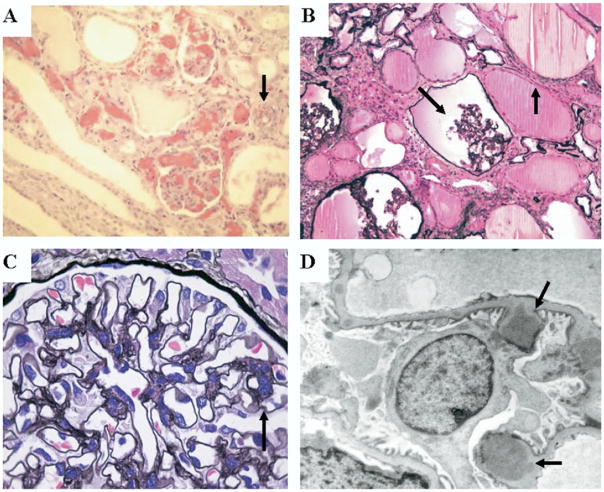
Representative photomicrographs of renal sections from children with HIV-HUS, HIVAN, and HIVICK. (A) Light microscopy renal section from a child with HIV-HUS showing collapsed glomerular capillary loops with red blood cell fragments and tubular microcysts. The black arrow shows an arteriole with luminal narrowing owing to red cell fragments and intramural thrombosis (hematoxylin-eosin stain, 200×). (B) Light microscopy renal section from a child with HIVAN. The black arrows show a shrunken glomerulus and microcystic tubular dilatation (Jones methenamine silver stain, 200×). Figure 2B courtesy of Dr. William Bates and Dr. Peter Nourse. (C) Light microscopy renal section from a child with HIVICK showing mesangial prominence. The glomerular tuft is lobulated with double contours of the glomerular basement membrane (black arrow) (Jones methenamine silver stain, 700×). (D) Transmission electron microscopy from a glomerular capillary in a child with HIVICK. The black arrows show subepithelial deposits (4.000×). Figure 2C and D courtesy of Drs. Stewart Goetch and Professor Udai Kala.
References
-
- UNAIDS. AIDS epidemic update. 2007. Available from: www.unaids.org/en/KnowledgeCentre/HIVData/EpiUpdate/EpiUpdArchive/2007/
-
- Ray PE, Rakusan TM, Loechelt BJ, Selby DM, Liu X-H, Chandra RS. Human immunodeficiency virus (HIV)-associated nephropathy in the children from the Washington D.C. area; 12 Years’ experience. Semin Nephrol. 1998;18:396–05. - PubMed
-
- Benson C, Kaplan J, Masur H. Treating opportunistic infections among HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America. Clin Infect Dis. 2005;40 (Suppl 1):S1–84. - PubMed
-
- McCulloch MI. Introduction to pediatric HIV disease [abstract] Pediatr Nephrol. 2007;22:1438, 298.
-
- Kala U, Petersen K, Faller G, Goetsch S. Spectrum of severe renal disease in children with HIV/Aids at Chris Hani Baragwanath Hospital, Johannesburg [abstract] Pediatr Nephrol. 2007;22:1439, 301.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
