

Effect of body posture on pharyngeal shape and size in adults with and without obstructive sleep apnea
- PMID: 19014074
- PMCID: PMC2579983
- DOI: 10.1093/sleep/31.11.1543
Effect of body posture on pharyngeal shape and size in adults with and without obstructive sleep apnea
Abstract
Study objectives: In patients with obstructive sleep apnea (OSA), the severity and frequency of respiratory events is increased in the supine body posture compared with the lateral recumbent posture. The mechanism responsible is not clear but may relate to the effect of posture on upper airway shape and size. This study compared the effect of body posture on upper airway shape and size in individuals with OSA with control subjects matched for age, BMI, and gender.
Participants: 11 males with OSA and 11 age- and BMI-matched male control subjects.
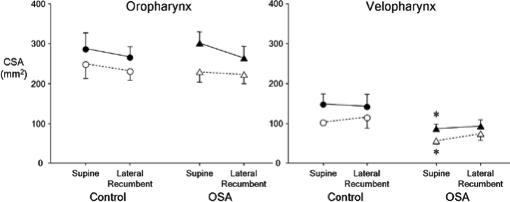
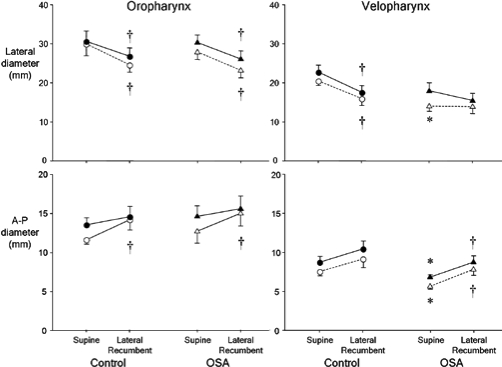
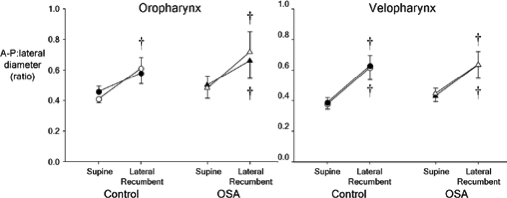
Results: Anatomical optical coherence tomography was used to scan the upper airway of all subjects while awake and breathing quietly, initially when supine, and then in the lateral recumbent posture. A standard head, neck, and tongue position was maintained during scanning. Airway cross-sectional area (CSA) and anteroposterior (A-P) and lateral diameters were obtained in the oropharyngeal and velopharyngeal regions in both postures. A-P to lateral diameter ratios provided an index of regional airway shape. In equivalent postures, the ratio of A-P to lateral diameter in the velopharynx was similar in OSA and control subjects. In both groups, this ratio was significantly less for the supine than for the lateral recumbent posture. CSA was smaller in OSA subjects than in controls but was unaffected by posture.
Conclusions: The upper airway changes from a more transversely oriented elliptical shape when supine to a more circular shape when in the lateral recumbent posture but without altering CSA. Increased circularity decreases propensity to tube collapse and may account for the postural dependency of OSA.
Figures


References
-
- Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7:110–4. - PubMed
-
- Oksenberg A. Positional vs nonpositional obstructive sleep apnea patients: anthropomorphic, nocturnal polysomnographic, and multiple sleep latency test data. Chest. 1997;112:629–39. - PubMed
-
- Oksenberg A. Association of body position with severity of apneic events in patients with severe nonpositional obstructive sleep apnea. Chest. 2000;118:1018–24. - PubMed
-
- Oksenberg A. The sleep supine position has a major effect on optimal nasal continuous positive airway pressure: relationship with rapid eye movements and non-rapid eye movements sleep, body mass index, respiratory disturbance index, and age. Chest. 1999;116:1000–6. - PubMed
-
- Boudewyns A, et al. Abbreviated method for assessing upper airway function in obstructive sleep apnea. Chest. 2000;118:1031–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
