

Assessment of sleep in ventilator-supported critically III patients
- PMID: 19014076
- PMCID: PMC2579984
- DOI: 10.1093/sleep/31.11.1559
Assessment of sleep in ventilator-supported critically III patients
Abstract
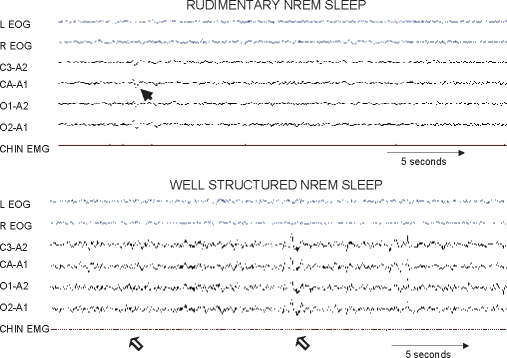
Objectives: In critically ill patients, sleep derangements are reported to be severe using Rechtschaffen and Kales (R&K) methodology; however, whether such methodology can reliably assess sleep during critical illness is unknown. We set out to determine the reproducibility of 4 different sleep-assessment methods (3 manual and 1 computer-based) for ventilator-supported critically ill patients and also to quantify the extent to which the reproducibility of the manual methods for measuring sleep differed between critically ill and ambulatory (control) patients.
Design: Observational methodologic study.
Setting: Academic center.
Patients: Critically ill patients receiving mechanical ventilation and age-matched controls underwent polysomnography.
Interventions: None.
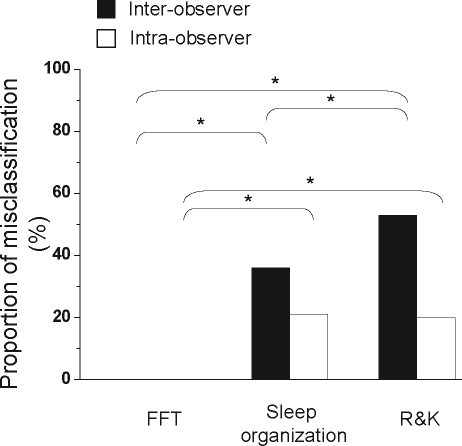
Measurements and results: Reproducibility for the computer-based method (spectral analysis of electroencephalography [EEG]) was better than that for the manual methods: R&K methodology and sleep-wakefulness organization pattern (P = 0.03). In critically ill patients, the proportion of misclassifications for measurements using spectral analysis, sleep-wakefulness organization pattern, and R&K methodology were 0%, 36%, and 53%, respectively (P < 0.0001). The EEG pattern of burst suppression was not observed. Interobserver and intraobserver reliability of the manual sleep-assessment methods for critically ill patients (kappa = 0.52 +/- 0.23) was worse than that for control patients (kappa = 0.89 +/- 0.13; P = 0.03). In critically ill patients, the overall reliability of the R&K methodology was relatively low for assessing sleep (kappa = 0.19), but detection of rapid eye movement sleep revealed good agreement (kappa = 0.70).
Conclusions: Reproducibility for spectral analysis of EEG was better than that for the manual methods: R&K methodology and sleep-wakefulness organization pattern. For assessment of sleep in critically ill patients, the use of spectral analysis, sleep-wakefulness organization state, or rapid eye movement sleep alone may be preferred over the R&K methodology.
Figures




References
-
- Gottlieb DJ, et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study. Sleep. 2006;29:1009–14. - PubMed
-
- Lorenzi-Filho G. Obstructive sleep apnea and atherosclerosis: a new paradigm. Am J Respir Crit Care Med. 2007;175:1219–21. - PubMed
-
- Parthasarathy S. Sleep in the intensive care unit. Intensive Care Med. 2004;30:197–206. - PubMed
-
- Leung RS. Sleep apnea and cardiovascular disease. Am J Respir Crit Care Med. 2001;164:2147–65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
