

doi: 10.1186/1757-1626-1-319.
Intraductal papillary mucinous tumor of bile ducts radiologic and pathologic features: a case report
Affiliations
- PMID: 19014697
- PMCID: PMC2613149
- DOI: 10.1186/1757-1626-1-319
Item in Clipboard
Intraductal papillary mucinous tumor of bile ducts radiologic and pathologic features: a case report
Cases J.
.
Abstract
We report a case of a 67-year-old Caucasian man with right upper quadrant abdominal pain. He underwent radiologic investigations that revealed a solid, focal mass, at the V hepatic segment. Because a definitive diagnosis, based on imaging appearance of the lesion, was impossible in our case, we performed a hystopathological investigation but the biopsies were inconclusive. So, the definitive diagnosis of intraductal papillary mucinous tumor of bile ducts was made on surgical resected material.Intraductal papillary neoplasm of the liver (IPNL) is a recently recognized entity which closely resembles an intraductal papillary mucinous tumor (IPMT) of the pancreas.
Figures

Transverse CT scan. It reveals a solid focal mass, about 3 cm in diameter, hypodense respect to the surrounding tissue in the basal phase (1) with a light peripherical enhanced rim in the arterial phase (2) that increases in the portal venous phase (3). In late phase (4), the lesion shows a puntacte aspect because of the presence of intralesional hypervascular spots (arrow). The bile ducts are not dilatated.

Transverse CT scan. It reveals a solid focal mass, about 3 cm in diameter, hypodense respect to the surrounding tissue in the basal phase (1) with a light peripherical enhanced rim in the arterial phase (2) that increases in the portal venous phase (3). In late phase (4), the lesion shows a puntacte aspect because of the presence of intralesional hypervascular spots (arrow). The bile ducts are not dilatated.

Transverse CT scan. It reveals a solid focal mass, about 3 cm in diameter, hypodense respect to the surrounding tissue in the basal phase (1) with a light peripherical enhanced rim in the arterial phase (2) that increases in the portal venous phase (3). In late phase (4), the lesion shows a puntacte aspect because of the presence of intralesional hypervascular spots (arrow). The bile ducts are not dilatated.

Transverse CT scan. It reveals a solid focal mass, about 3 cm in diameter, hypodense respect to the surrounding tissue in the basal phase (1) with a light peripherical enhanced rim in the arterial phase (2) that increases in the portal venous phase (3). In late phase (4), the lesion shows a puntacte aspect because of the presence of intralesional hypervascular spots (arrow). The bile ducts are not dilatated.

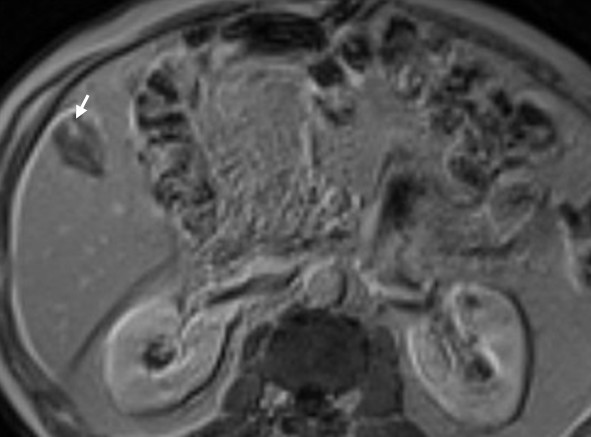
Transverse RM scan. It reveals a slightly dishomogeneous hyperintense mass in sequences with long TR (5) and the appearance of intralesional hypervascular spots (arrow) in late phase after administration of paramagnetic contrast agent (6).
Transverse RM scan. It reveals a slightly dishomogeneous hyperintense mass in sequences with long TR (5) and the appearance of intralesional hypervascular spots (arrow) in late phase after administration of paramagnetic contrast agent (6).

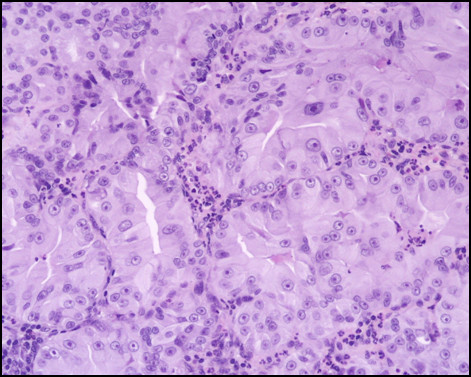
Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.

Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.
Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.

Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.

Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.

Pathological sections specimens. (7) Low magnification showing encapsulated papillary tumor with thin fibrovascular stalk, covered by tall mucinous moderately dysplastic epithelium (8). Higher magnification demonstrates area with oncocitic pattern (9). The immunohistochemical test showed a diffuse CK7+ (10) and apomucines MUC5AC (11) and MUC6 (12) positivity in more than 50% of neoplastic cells.

CT follow up examination. It shows the patient free of the disease.
Similar articles
-
Cyst-forming intraductal papillary neoplasm of the bile ducts: description of imaging and pathologic aspects.AJR Am J Roentgenol. 2011 Nov;197(5):1111-20. doi: 10.2214/AJR.10.6363. AJR Am J Roentgenol. 2011. PMID: 22021503
-
A case of intraductal papillary neoplasm of the bile duct accompanied by intraductal papillary mucinous neoplasm of the pancreas and hepatocellular carcinoma.Clin J Gastroenterol. 2021 Oct;14(5):1536-1543. doi: 10.1007/s12328-021-01461-z. Epub 2021 Jun 9. Clin J Gastroenterol. 2021. PMID: 34106396
-
Endoscopic ultrasound-guided fine needle aspiration cytology of intraductal papillary mucinous tumor of the pancreas. A case report.Acta Cytol. 2003 Jul-Aug;47(4):657-62. doi: 10.1159/000326584. Acta Cytol. 2003. PMID: 12920762
-
Mucin-producing neoplasms of the pancreas. Intraductal papillary and mucinous cystic neoplasms.Ann Surg. 1996 Feb;223(2):141-6. doi: 10.1097/00000658-199602000-00005. Ann Surg. 1996. PMID: 8597507 Free PMC article. Review.
-
Intraductal papillary mucininous neoplasm of the bile ducts: multimodality assessment with pathologic correlation.Abdom Imaging. 2011 Aug;36(4):447-56. doi: 10.1007/s00261-010-9649-x. Abdom Imaging. 2011. PMID: 20959978 Review.
Cited by
-
Surgical Treatment of Intraductal Papillary Neoplasm of the Bile Duct: A Report of Two Cases and Review of the Literature.Front Oncol. 2022 Jun 23;12:916457. doi: 10.3389/fonc.2022.916457. eCollection 2022. Front Oncol. 2022. PMID: 35814451 Free PMC article.
References
-
- Lim JH. Cholangiocarcinoma: morphologic classification according to growth pattern and imaging findings. AJR Am J Roentgenol. 2003;181:819–827. - PubMed
