

Female genital cutting: a persisting practice
- PMID: 19015765
- PMCID: PMC2582648
Female genital cutting: a persisting practice
Abstract
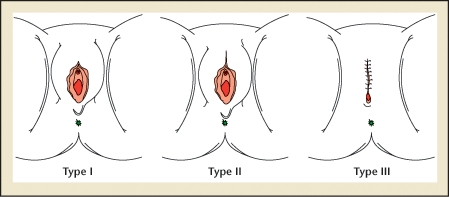
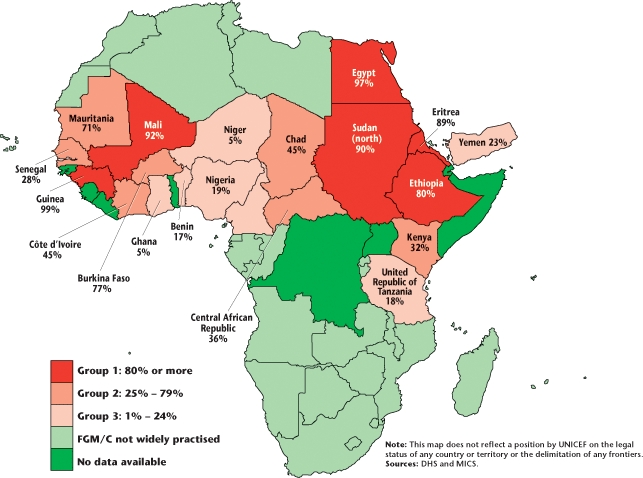
More than 130 million women worldwide have undergone female genital cutting (FGC). FGC occurs in parts of Africa and Asia, in societies with various cultures and religions. Reasons for the continuing practice of FGC include rite of passage, preserving chastity, ensuring marriageability, religion, hygiene, improving fertility, and enhancing sexual pleasure for men. The World Health Organization has classified FGC into 4 types depending on the extent of tissue removed. Immediate complications include hemorrhage, infection, sepsis, and death. Long-term complications include pain, scarring, urinary issues, and poor obstetric and neonatal outcomes. Efforts are being made nationally and internationally to eradicate this practice.
Keywords: Female circumcision; Female genital cutting; Female genital mutilation.
Figures
References
-
- Female Genital Mutilation: A Joint WHO/UNICEF/UNFPA Statement. Geneva, Switzerland: World Health Organization; 1997.
-
- Female genital mutilation (FGM) [Accessed September 2, 2008]. World Health Organization Web site. http://www.who.int/reproductive-health/fgm/index.html.
-
- Eliminating Female Genital Mutilation: An Interagency Statement. Geneva, Switzerland: World Health Organization; 2008.
-
- Nour N. Female genital cutting: clinical and cultural guidelines. Obstet Gynecol Surv. 2004;59:272–279. - PubMed
-
- Mandara M. Female genital mutilation in Nigeria. Int J Gynaecol Obstet. 2004;84:291–298. - PubMed
LinkOut - more resources
Full Text Sources