

Cognitive functioning during highly active antiretroviral therapy interruption in human immunodeficiency virus type 1 infection
- PMID: 19016380
- PMCID: PMC4692591
- DOI: 10.1080/13550280802372313
Cognitive functioning during highly active antiretroviral therapy interruption in human immunodeficiency virus type 1 infection
Abstract
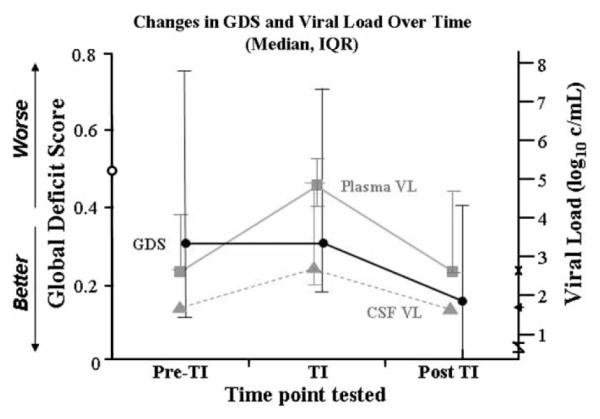
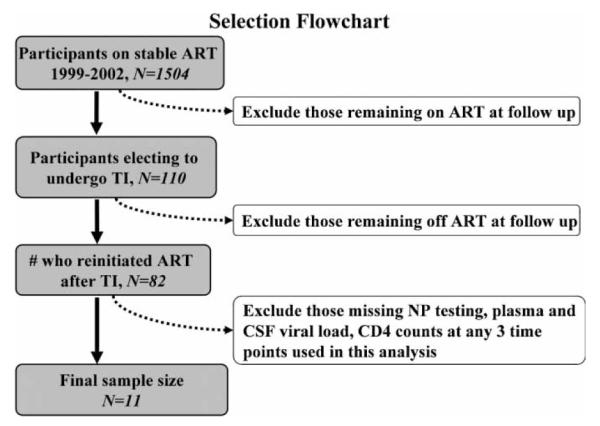
Although no longer considered therapeutically beneficial, antiretroviral treatment interruptions (TIs) still occur frequently among patients with human immunodeficiency virus (HIV) infection for a variety of reasons. TIs typically result in viral rebound and worsening immunosuppression, which in turn are risk factors for neurocognitive decline and dementia. We sought to determine the extent of neurocognitive risk with TIs and subsequent reintroduction of highly active antiretroviral therapy (HAART) by using a comprehensive, sensitive neuropsychological assessment and by concurrently determining changes in plasma and cerebrospinal fluid (CSF) viral load and CD4 counts. Prospective, serial, clinical evaluations including neuropsychological (NP) testing and measurement of plasma HIV RNA and CD4 count and mood state were performed on HIV-1-infected individuals (N=11) at three time points: (1) prior to a TI, while on HAART; (2) after TIs averaging 6 months; and (3) after reinitiating HAART therapy. During TI, plasma HIV RNA increased and CD4 counts declined significantly, but NP performance did not change. Following reinitiation of HAART, viral loads fell below pre-TI levels, and CD4 counts rose. Improved viral suppression and immune restoration with reinitiation of HAART resulted in significant improvement in neurocognitive performance. No changes on comprehensive questionnaires of mood state were observed in relation to TI.NP performance and mood state remained stable during TIs despite worsened viral loads and CD4 counts. Because "practice effects" are generally greatest between the first and second NP testing sessions, improvement at the third, post-TI time point was unlikely to be accounted for by practice. TIs of up to 6 months appear to be neurocognitively and psychiatrically safe for most patients.
Figures
References
-
- Beck A, Steer R, Brown G. BDI-II Beck Depression Inventory manual. Harcourt Brace and Company; San Antonio, TX: 1996.
-
- Benedict RH. Brief Visuospatial Memory Test—Revised. Psychological Assessments Resources; Odessa, TX: 1997.
-
- Benedict RH, Schretlen D, Groninger L, Brandt J. Hopkins Verbal Learning Test—Revised: normative data and analysis of inter-form and test-retest reliability. Clin Neuropsychologist. 1998;12:43–55.
-
- Benton A, Hamsher K, Sivan A. Multilingual aphasia examination. AJA Associates; Iowa City, IA: 1994.
-
- Carey CL, Woods SP, Gonzalez R, Conover E, Marcotte TD, Grant I, Heaton RK. Predictive validity of global deficit scores in detecting neuropsychological impairment in HIV infection. J Clin Exp Neuropsychol. 2004;26:307–319. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
