

Antisense hypoxia-inducible factor 1alpha gene therapy enhances the therapeutic efficacy of doxorubicin to combat hepatocellular carcinoma
- PMID: 19016766
- PMCID: PMC11159667
- DOI: 10.1111/j.1349-7006.2008.00905.x
Antisense hypoxia-inducible factor 1alpha gene therapy enhances the therapeutic efficacy of doxorubicin to combat hepatocellular carcinoma
Abstract
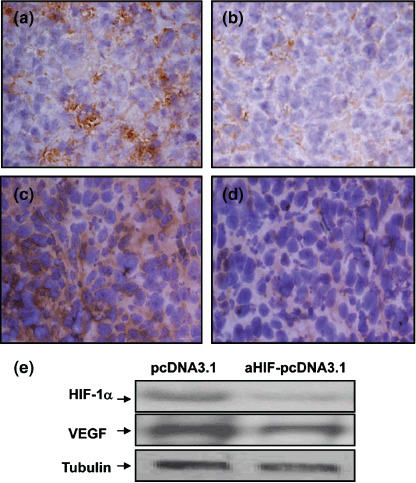
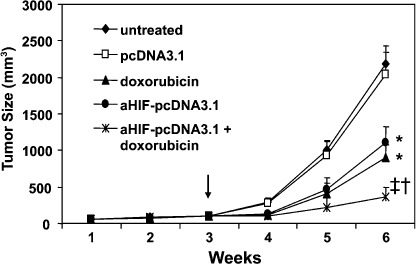
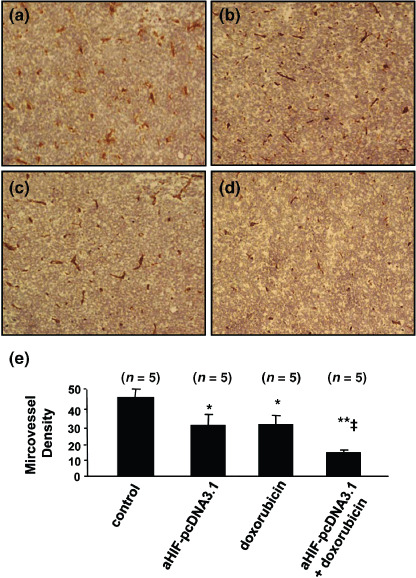
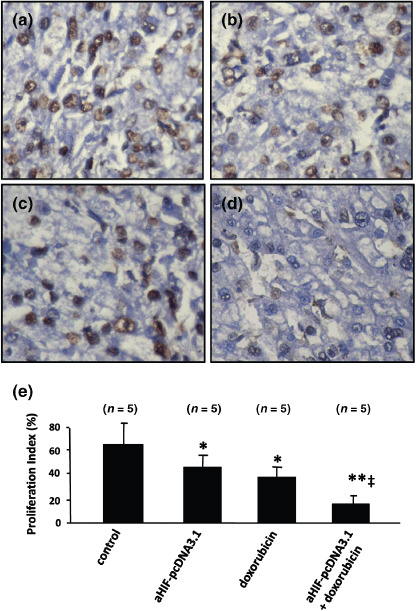
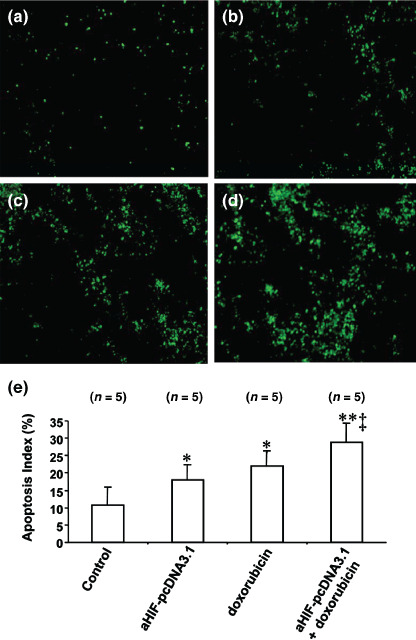
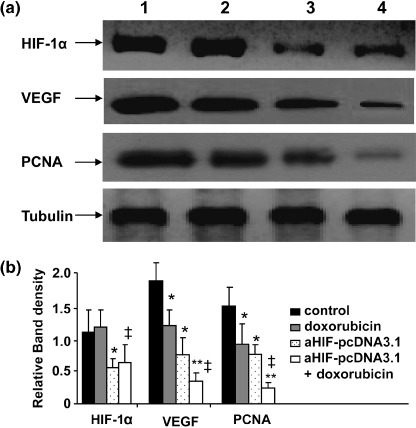
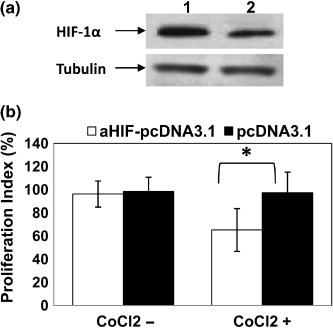
Hepatocellular carcinoma (HCC), one of the most common cancers worldwide, is resistant to anticancer drugs. Hypoxia is a major cause of tumor resistance to chemotherapy, and hypoxia-inducible factor (HIF)-1 is a key transcription factor in hypoxic responses. We have previously demonstrated that gene transfer of an antisense HIF-1alpha expression vector downregulates expression of HIF-1alpha and vascular endothelial growth factor (VEGF), and synergizes with immunotherapy to eradicate lymphomas. The aim of the present study was to determine whether gene transfer of antisense HIF-1alpha could enhance the therapeutic efficacy of doxorubicin to combat HCC. Both antisense HIF-1alpha therapy and doxorubicin suppressed the growth of subcutaneous human HepG2 tumors established in BALB/c nude mice, tumor angiogenesis, and cell proliferation, and induced tumor cell apoptosis. The combination therapy with antisense HIF-1alpha and doxorubicin was more effective in suppressing tumor growth, angiogenesis, and cell proliferation, and inducing cell apoptosis than the respective monotherapies. Gene transfer of antisense HIF-1alpha downregulated the expression of both HIF-1alpha and VEGF, whereas doxorubicin only downregulated VEGF expression. Antisense HIF-1alpha and doxorubicin synergized to downregulate VEGF expression. Both antisense HIF-1alpha and doxorubicin inhibited expression of proliferating cell nuclear antigen, and combined to exert even stronger inhibition of proliferating cell nuclear antigen expression. Antisense HIF-1alpha therapy warrants investigation as a therapeutic strategy to enhance the efficacy of doxorubicin for treating HCC.
Figures
References
-
- Befeler AS, Di Bisceglie AM. Hepatocellular carcinoma: diagnosis and treatment. Gastroenterology 2002; 122: 1609–19. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74–108. - PubMed
-
- Zhu AX. Systemic therapy of advanced hepatocellular carcinoma: how hopeful should we be? Oncologist 2006; 11: 790–800. - PubMed
-
- Sciarrino E, Simonetti RG, Le Moli S et al . Adriamycin treatment for hepatocellular carcinoma. Experience with 109 patients. Cancer 1985; 56: 2751–5. - PubMed
-
- Nerenstone SR, Ihde DC, Friedman MA. Clinical trials in primary hepatocellular carcinoma: current status and future directions. Cancer Treat Rev 1988; 15: 1–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
