

Case Reports
doi: 10.1111/j.1349-7006.2008.00958.x.
Acute tumor lysis syndrome after transarterial chemoembolization for hepatocellular carcinoma
Affiliations
- PMID: 19016772
- PMCID: PMC11158201
- DOI: 10.1111/j.1349-7006.2008.00958.x
Item in Clipboard
Case Reports
Acute tumor lysis syndrome after transarterial chemoembolization for hepatocellular carcinoma
Cancer Sci.
2008 Oct.
Abstract
A 77-year-old-man was admitted to hospital for treatment of a huge hepatocellular carcinoma by transarterial chemoembolization. After treatment, the patient developed acute tumor lysis syndrome with hyperkalemia, hyperuricemia, hyperphosphatemia, hypocalcemia, metabolic acidosis and acute renal failure, which was successfully treated. In the treatments of solid organ tumors, acute tumor lysis syndrome is an extremely rare complication. To the best of the authors' knowledge, this patient is the third case of such a complication after transarterial chemoembolization for a hepatocellular carcinoma in the English literature.
Figures
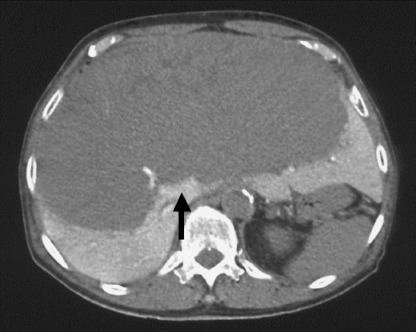
Computed tomography during arterial portography before transarterial chemoembolization revealed a huge hepatocellular carcinoma (arrow) occupying both hepatic lobes.
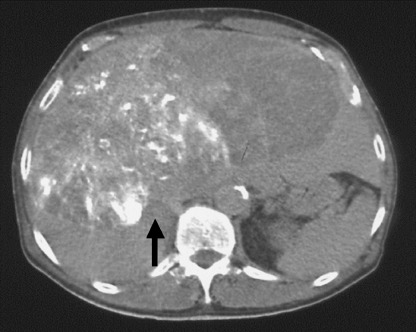
Plain computed tomography after transarterial chemoembolization revealed iodized oil esters accumulation (arrow) in the huge hepatocellular carcinoma of the right hepatic lobe.
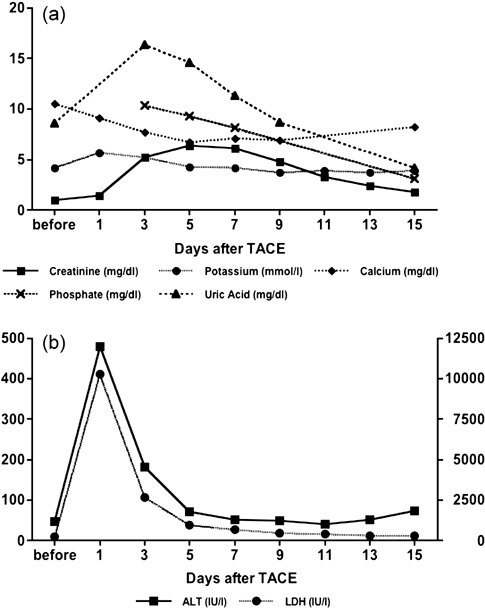
Changes in laboratory data of metabolic profiles and liver function after transarterial chemoembolization (TACE). (a) Y‐axis shows values of creatinine (mg/dL), potassium (mmol/L), calcium (mg/dL), phosphate (mg/dL) and uric acid (mg/dL). (b) Y‐axis shows values of alanine aminotransferase (IU/L) and YY‐axis shows values of lactate dehydrogenase (IU/L). All laboratory data was improved by intravenous hydration with sodium bicarbonate and administration of allopurinol.
References
-
- Brereton HD, Anderson T, Johnson RE, Schein PS. Hyperphosphatemia and hypocalcemia in Burkitt lymophoma: complications of chemotherapy. Arch Intern Med 1975; 135: 307–9. - PubMed
-
- Cadman EC, Lunberg WB, Bertino JR. Hyperphosphatermia and hypocalcemia accompanying rapid cell lysis in a patient with Burkitt's lymphoma and Burkitt cell leukemia. Am J Med 1977; 62: 283–90. - PubMed
-
- Zusman J, Brown DM, Nesbit ME. Hyperphosphatemia, hyperphosphaturia and hypocalcemia in acute lymphoblastic leukemia. N Engl J Med 1973; 289: 1335–40. - PubMed
-
- Boles JM, Dutel JL, Briere J et al . Acute renal failure caused by extreme hyperphosphatemia after chemotherapy of an acute lymphoblastic leukemia. Cancer 1984; 53: 2425–9. - PubMed
-
- Tsokos GC, Balow JE, Spiegel RJ, Magrath IT. Renal and metabolic complications of undifferentiated and lymphoblastic lymphomas. Medicine 1981; 60: 218–29. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
