

Phenylephrine versus norepinephrine for initial hemodynamic support of patients with septic shock: a randomized, controlled trial
- PMID: 19017409
- PMCID: PMC2646303
- DOI: 10.1186/cc7121
Phenylephrine versus norepinephrine for initial hemodynamic support of patients with septic shock: a randomized, controlled trial
Abstract
Introduction: Previous findings suggest that a delayed administration of phenylephrine replacing norepinephrine in septic shock patients causes a more pronounced hepatosplanchnic vasoconstriction as compared with norepinephrine. Nevertheless, a direct comparison between the two study drugs has not yet been performed. The aim of the present study was, therefore, to investigate the effects of a first-line therapy with either phenylephrine or norepinephrine on systemic and regional hemodynamics in patients with septic shock.
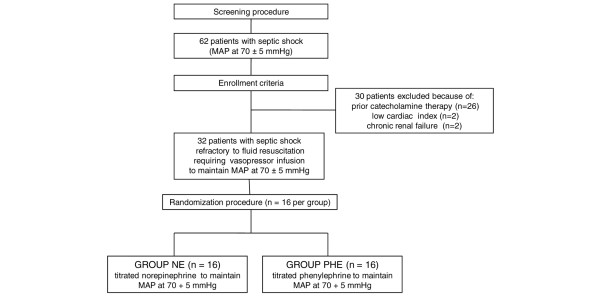
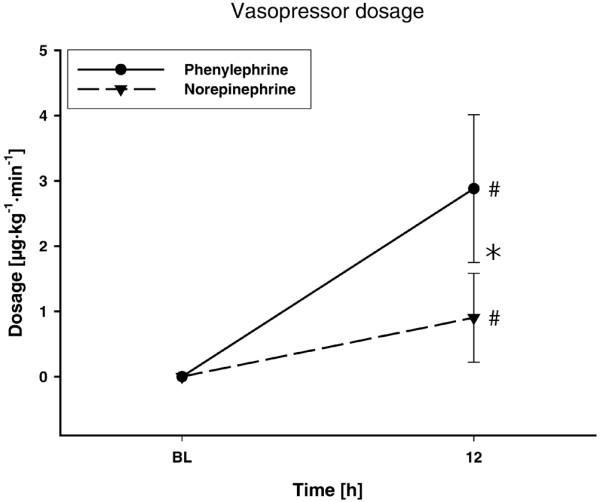
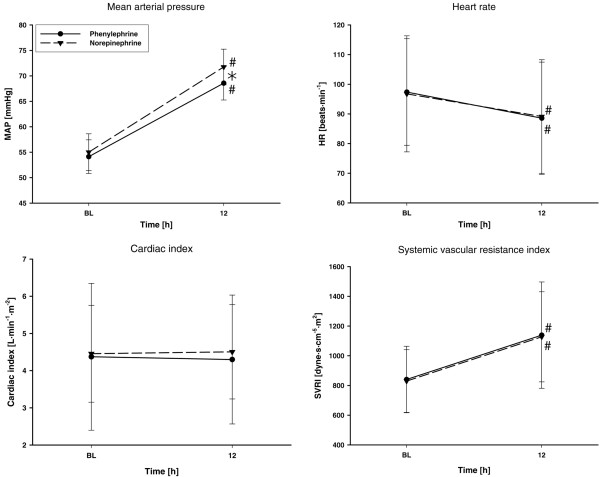
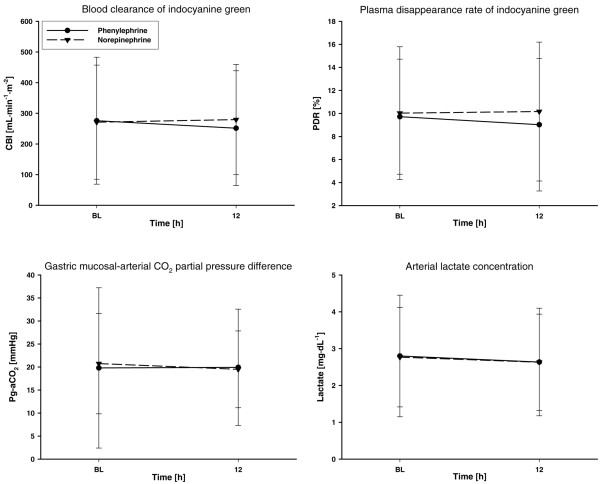
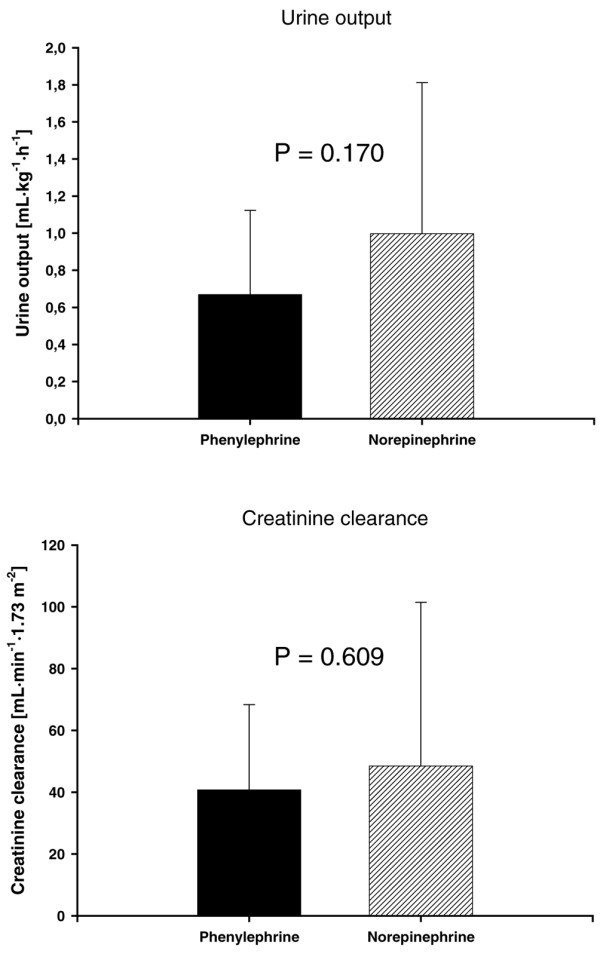
Methods: We performed a prospective, randomized, controlled trial in a multidisciplinary intensive care unit in a university hospital. We enrolled septic shock patients (n = 32) with a mean arterial pressure below 65 mmHg despite adequate volume resuscitation. Patients were randomly allocated to treatment with either norepinephrine or phenylephrine infusion (n = 16 each) titrated to achieve a mean arterial pressure between 65 and 75 mmHg. Data from right heart catheterization, a thermodye dilution catheter, gastric tonometry, acid-base homeostasis, as well as creatinine clearance and cardiac troponin were obtained at baseline and after 12 hours. Differences within and between groups were analyzed using a two-way analysis of variance for repeated measurements with group and time as factors. Time-independent variables were compared with one-way analysis of variance.
Results: No differences were found in any of the investigated parameters.
Conclusions: The present study suggests there are no differences in terms of cardiopulmonary performance, global oxygen transport, and regional hemodynamics when phenylephrine was administered instead of norepinephrine in the initial hemodynamic support of septic shock.
Trial registration: ClinicalTrial.gov NCT00639015.
Figures
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Taylor Thompson B, Townsend S, Vender JS, Zimmerman JL, Vincent JL. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. doi: 10.1097/CCM.0b013e31817d7ee4. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
