

Predicting aspiration in patients with ischemic stroke: comparison of clinical signs and aerodynamic measures of voluntary cough
- PMID: 19017886
- PMCID: PMC3121155
- DOI: 10.1378/chest.08-1122
Predicting aspiration in patients with ischemic stroke: comparison of clinical signs and aerodynamic measures of voluntary cough
Abstract
Background: Clinical signs often fail to identify stroke patients who are at increased risk of aspiration. We hypothesized that objective measure of voluntary cough would improve the accuracy of the clinical evaluation of swallow to predict those patients who are at risk.
Methods: A comprehensive diagnostic evaluation was completed for 96 consecutive stroke patients that included cognitive testing, a bedside clinical swallow examination, aerodynamic and sound pressure level measures of voluntary cough, and "gold standard" instrumental swallowing studies (ie, videofluoroscopic evaluation of swallow [VSE] or fiberoptic endoscopic evaluation of swallow [FEES]). Stroke severity was assessed retrospectively using the Canadian neurologic scale.
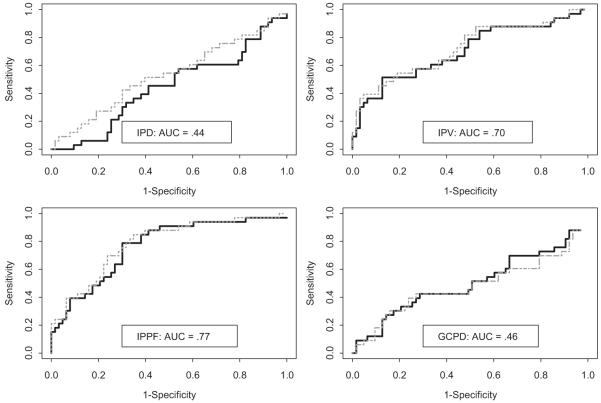
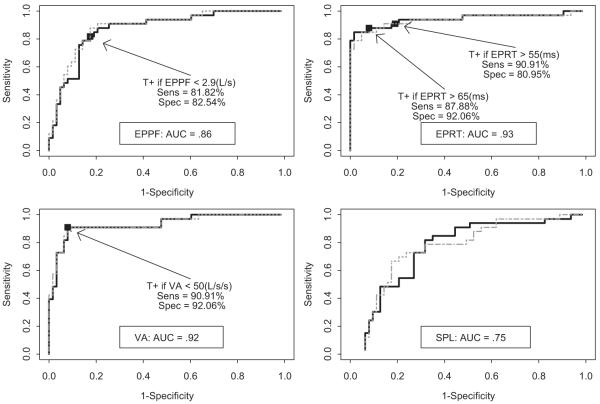
Results: Based on the findings of VSE/FEES, 33 patients (34%) were at high risk of aspiration and (66%) were nonaspirators. Clinical signs (eg, absent swallow, difficulty handling secretions, or reflexive cough after water bolus) had an overall accuracy of 74% with a sensitivity of 58% and a specificity of 83% for the detection of aspiration. Three objective measures of voluntary cough (expulsive phase rise time, volume acceleration, and expulsive phase peak flow) were each associated with an aspiration risk category (areas under the curves were 0.93, 0.92, and 0.86, respectively). Expulsive phase rise time > 55 m/s, volume acceleration < 50 L/s/s, and expulsive phase peak flow < 2.9 L/s had sensitivities of 91%, 91%, and 82%, respectively; and specificities of 81%, 92%, and 83%, respectively for the identification of aspirators.
Conclusion: Objective measures of voluntary cough can identify stroke patients who are at risk for aspiration and may be useful as an adjunct to the standard bedside clinical assessment.
Figures
Comment in
-
Cough and aspiration.Chest. 2009 Aug;136(2):647-648. doi: 10.1378/chest.09-0199. Chest. 2009. PMID: 19666771 No abstract available.
References
-
- Doggett DL, Tappe KA, Mitchell MD, et al. Prevention of pneumonia in elderly stroke patients by systematic diagnosis and treatment of dysphagia: an evidence-based comprehensive analysis of the literature. Dysphagia. 2001;16:279–295. - PubMed
-
- Foley N, Finestone H, Woodbury MG, et al. Energy and protein intakes of acute stroke patients. J Nutr Health Aging. 2006;10:171–175. - PubMed
-
- Feinberg MJ, Ekberg O. Deglutition after near-fatal choking episode: radiologic evaluation. Radiology. 1990;176:637–640. - PubMed
-
- Daniels SK, Brailey K, Priestly DH, et al. Aspiration in patients with acute stroke. Arch Phys Med Rehabil. 1998;79:14–19. - PubMed
-
- Mann G, Dip PG, Hankey GJ, et al. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30:744–748. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
