

Elevated levels of the receptor for advanced glycation end products, a marker of alveolar epithelial type I cell injury, predict impaired alveolar fluid clearance in isolated perfused human lungs
- PMID: 19017890
- PMCID: PMC2714162
- DOI: 10.1378/chest.08-0919
Elevated levels of the receptor for advanced glycation end products, a marker of alveolar epithelial type I cell injury, predict impaired alveolar fluid clearance in isolated perfused human lungs
Abstract
Background: Although alveolar epithelial injury is a major determinant of outcome in patients with acute lung injury, there is no reliable biological marker of alveolar epithelial injury. The primary objective was to determine whether elevated levels of the receptor for advanced glycation end products (RAGE), a marker of alveolar epithelial injury, reflect impaired alveolar fluid clearance (AFC) in an ex vivo perfused human lung preparation. A second objective was to determine whether levels of a marker of endothelial injury, von Willebrand factor antigen (vWF:Ag), are associated with impaired AFC.
Methods: Human lungs (N = 30) declined for transplantation by the California Transplant Donor Network were perfused at a constant pulmonary artery pressure of 12 mm Hg. Following rewarming to 36 degrees C, the lungs were inflated with a continuous positive airway pressure of 10 cm H(2)O. RAGE and vWF:Ag levels and AFC rates were then measured.
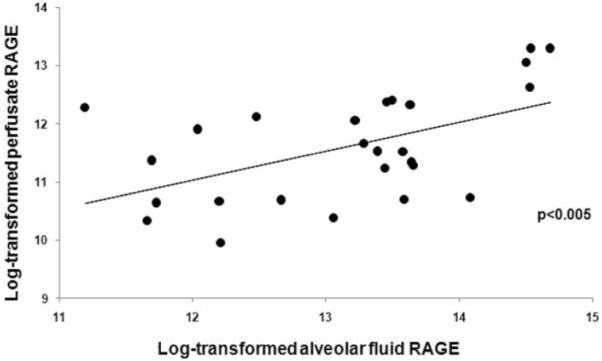
Results: The rate of AFC was inversely correlated with RAGE levels in the alveolar fluid (p < 0.005). Similarly, the concentration of RAGE in the alveolar fluid was significantly higher in lungs with submaximal AFC, defined in a prespecified analysis as <or= 14%/h, when compared with lungs with preserved AFC (median 0.82 vs 0.43 microg/mL; p < 0.05). In contrast, vWF:Ag levels did not correlate with the rate of AFC.
Conclusions: RAGE may be a useful biological marker of alveolar epithelial injury and impaired AFC in donor lungs prior to transplant and perhaps in patients with acute lung injury.
Figures




References
-
- Ware LB, Wang Y, Fang X, et al. Assessment of lungs rejected for transplantation and implications for donor selection. Lancet. 2002;360:619–620. - PubMed
-
- Steen S, Sjoberg T, Pierre L, et al. Transplantation of lungs from a non-heart-beating donor. Lancet. 2001;357:825–829. - PubMed
-
- de Antonio DG, Marcos R, Laporta R, et al. Results of clinical lung transplant from uncontrolled non-heart-beating donors. J Heart Lung Transplant. 2007;26:529–534. - PubMed
-
- Steen S, Ingemansson R, Eriksson L, et al. First human transplantation of a nonacceptable donor lung after reconditioning ex vivo. Ann Thorac Surg. 2007;83:2191–2194. - PubMed
-
- Ware LB, Matthay MA. Alveolar fluid clearance is impaired in the majority of patients with acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001;163:1376–1383. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
