

Estrogen receptor genotypes influence hot flash prevalence and composite score before and after tamoxifen therapy
- PMID: 19018086
- PMCID: PMC2645113
- DOI: 10.1200/JCO.2008.16.8377
Estrogen receptor genotypes influence hot flash prevalence and composite score before and after tamoxifen therapy
Abstract
Purpose: Hot flashes are common and frequently lead to drug discontinuation among women prescribed tamoxifen. We determined whether genetic polymorphisms in estrogen receptors (ESRs) alpha and beta (ESR1 and ESR2, respectively) are associated with tamoxifen-induced hot flashes.
Patients and methods: We determined ESR1 PvuII and XbaI and ESR2-02 genotypes in 297 women who were initiating tamoxifen. One-week hot flash diaries were collected to calculate a hot flash score (frequency x severity) before and 1, 4, 8, and 12 months after starting tamoxifen.
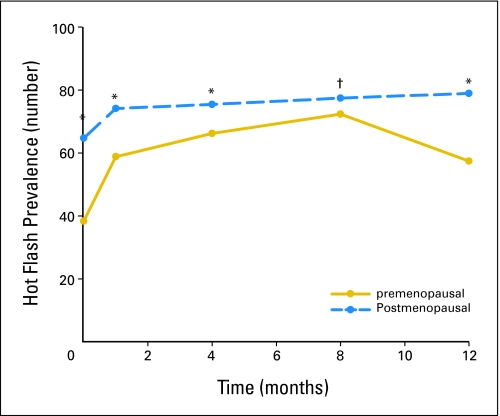
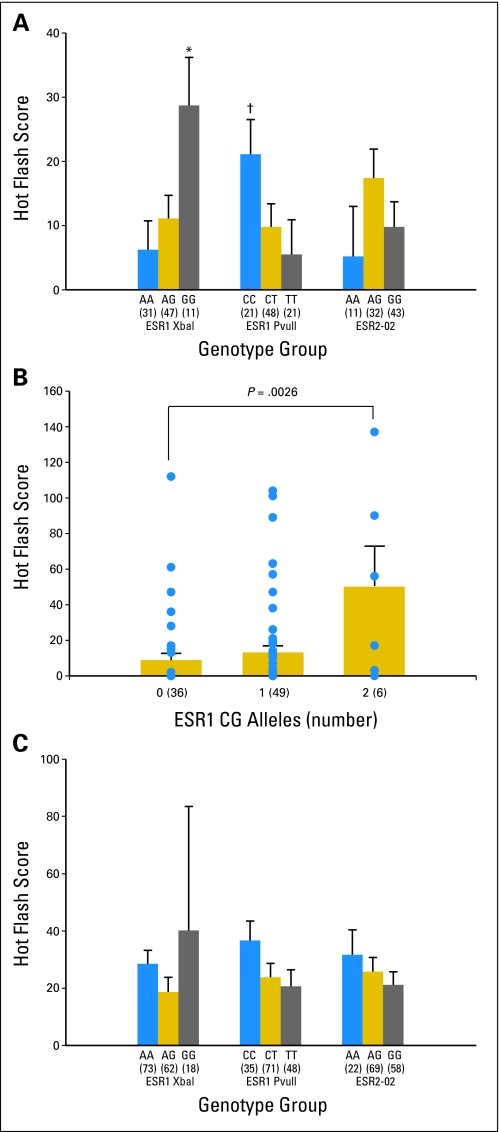
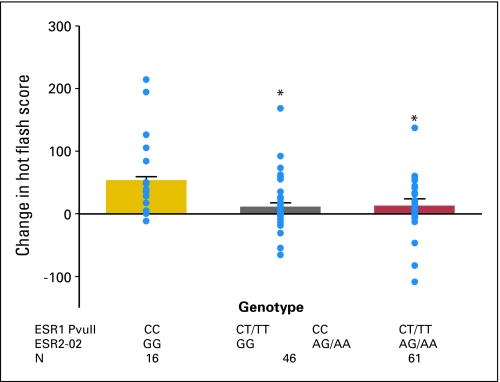
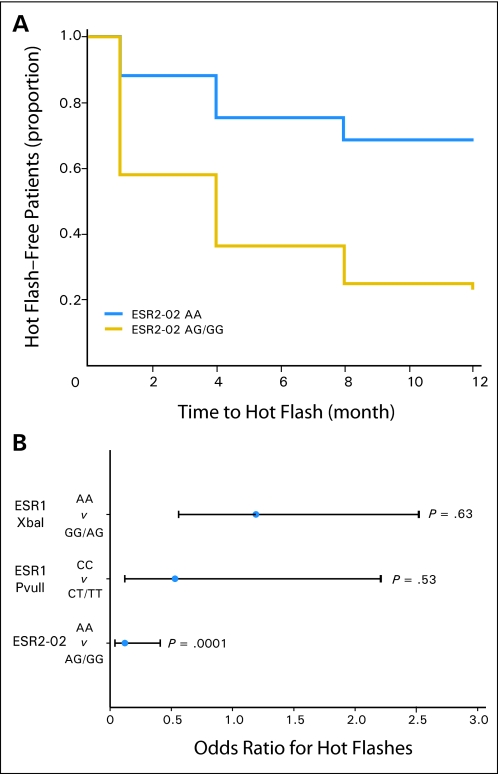
Results: Approximately 80% of 297 participants reported hot flashes before or during the first year of tamoxifen. After 4 months of tamoxifen, premenopausal women who did not receive adjuvant chemotherapy had a four-fold increase in hot flash score (from 5.9 to 23.6; P = .003) compared with a 1.17-fold increase (from 19.6 to 23; P = .34) in those who received chemotherapy. In premenopausal women, increased number of ESR1 PvuII and XbaI CG alleles was associated with higher baseline hot flash scores compared with those who had other haplotypes (P = .0026). At 4 months, postmenopausal women with ESR1 PvuII CC and ESR2-02 GG genotypes had 4.6 times increases in hot flash scores than other postmenopausal women (56 v 12; P = .0007). Women who had the ESR2-02 AA genotype were significantly less likely to experience tamoxifen-induced hot flashes than women who carried at least one ESR-02 G allele (hazard ratio, 0.26; 95% CI, 0.10 to 0.63; P = .001).
Conclusion: Knowledge of menopausal status, prior chemotherapy, and ESR genotype may help predict which women are most likely to suffer hot flashes during tamoxifen treatment.
Figures
Comment in
-
Gene testing to predict tamoxifen-induced hot flashes: new biological insights.J Clin Oncol. 2008 Dec 20;26(36):5841-2. doi: 10.1200/JCO.2008.19.5040. Epub 2008 Nov 17. J Clin Oncol. 2008. PMID: 19018077 No abstract available.
References
-
- Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 365:1687-1717, 2005 - PubMed
-
- Cuzick J, Powles T, Veronesi U, et al: Overview of the main outcomes in breast-cancer prevention trials. Lancet 361:296-300, 2003 - PubMed
-
- Stearns V, Ullmer L, Lopez JF, et al. Hot flushes. Lancet 360:1851-1861, 2002 - PubMed
-
- Day R: Quality of life and tamoxifen in a breast cancer prevention trial: A summary of findings from the NSABP P-1 study. Ann NY Acad Sci 949:143-150, 2001 - PubMed
-
- Fallowfield L: Acceptance of adjuvant therapy and quality of life issues. The Breast 14:612-616, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
