

Early antiretroviral therapy and mortality among HIV-infected infants
- PMID: 19020325
- PMCID: PMC2950021
- DOI: 10.1056/NEJMoa0800971
Early antiretroviral therapy and mortality among HIV-infected infants
Abstract
Background: In countries with a high seroprevalence of human immunodeficiency virus type 1 (HIV-1), HIV infection contributes significantly to infant mortality. We investigated antiretroviral-treatment strategies in the Children with HIV Early Antiretroviral Therapy (CHER) trial.
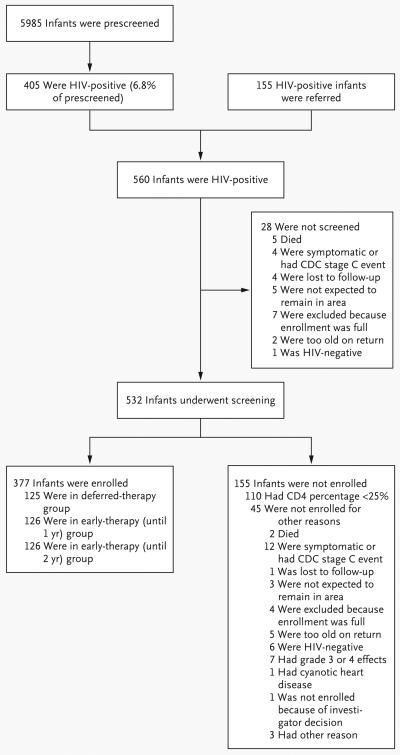
Methods: HIV-infected infants 6 to 12 weeks of age with a CD4 lymphocyte percentage (the CD4 percentage) of 25% or more were randomly assigned to receive antiretroviral therapy (lopinavir-ritonavir, zidovudine, and lamivudine) when the CD4 percentage decreased to less than 20% (or 25% if the child was younger than 1 year) or clinical criteria were met (the deferred antiretroviral-therapy group) or to immediate initiation of limited antiretroviral therapy until 1 year of age or 2 years of age (the early antiretroviral-therapy groups). We report the early outcomes for infants who received deferred antiretroviral therapy as compared with early antiretroviral therapy.
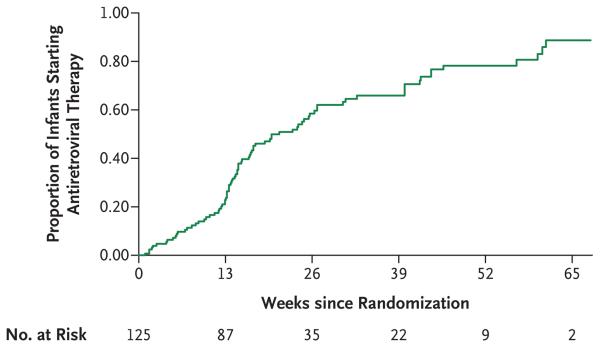
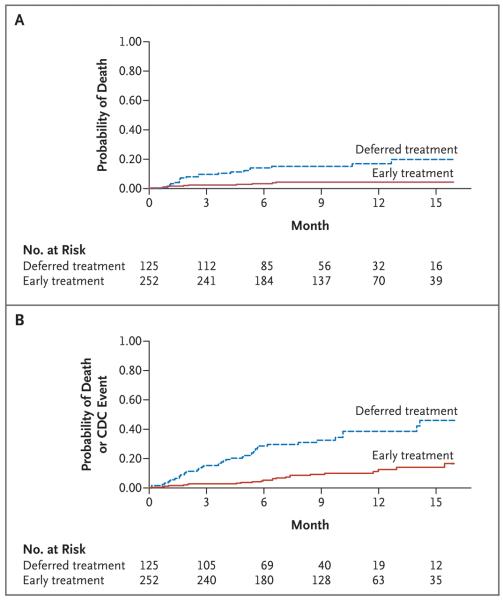
Results: At a median age of 7.4 weeks (interquartile range, 6.6 to 8.9) and a CD4 percentage of 35.2% (interquartile range, 29.1 to 41.2), 125 infants were randomly assigned to receive deferred therapy, and 252 infants were randomly assigned to receive early therapy. After a median follow-up of 40 weeks (interquartile range, 24 to 58), antiretroviral therapy was initiated in 66% of infants in the deferred-therapy group. Twenty infants in the deferred-therapy group (16%) died versus 10 infants in the early-therapy groups (4%) (hazard ratio for death, 0.24; 95% confidence interval [CI], 0.11 to 0.51; P<0.001). In 32 infants in the deferred-therapy group (26%) versus 16 infants in the early-therapy groups (6%), disease progressed to Centers for Disease Control and Prevention stage C or severe stage B (hazard ratio for disease progression, 0.25; 95% CI, 0.15 to 0.41; P<0.001). Stavudine was substituted for zidovudine in four infants in the early-therapy groups because of neutropenia in three infants and anemia in one infant; no drugs were permanently discontinued. After a review by the data and safety monitoring board, the deferred-therapy group was modified, and infants in this group were all reassessed for initiation of antiretroviral therapy.
Conclusions: Early HIV diagnosis and early antiretroviral therapy reduced early infant mortality by 76% and HIV progression by 75%. (ClinicalTrials.gov number, NCT00102960.)
2008 Massachusetts Medical Society
Figures
References
-
- Diaz C, Hanson C, Cooper ER, et al. Disease progression in a cohort of infants with vertically acquired HIV infection observed from birth: the Women and Infants Transmission Study (WITS) J Acquir Immune Defic Syndr Hum Retrovirol. 1998;18:221–8. - PubMed
-
- Tovo PA, de Martino M, Gabiano C, et al. Prognostic factors and survival in children with perinatal HIV-1 infection: the Italian register for HIV infections in children. Lancet. 1992;339:1249–53. - PubMed
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet. 2004;364:1236–43. - PubMed
-
- Dunn D. Short-term risk of disease progression in HIV-1-infected children receiving no antiretroviral therapy or zidovudine monotherapy: a meta-analysis. Lancet. 2003;362:1605–11. - PubMed
-
- Scaling up antiretroviral therapy in resource-limited settings: guidelines for a public health approach. World Health Organization; Geneva: 2002. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous