

Presence of electroencephalogram burst suppression in sedated, critically ill patients is associated with increased mortality
- PMID: 19020432
- PMCID: PMC3768119
- DOI: 10.1097/CCM.0b013e318186b9ce
Presence of electroencephalogram burst suppression in sedated, critically ill patients is associated with increased mortality
Abstract
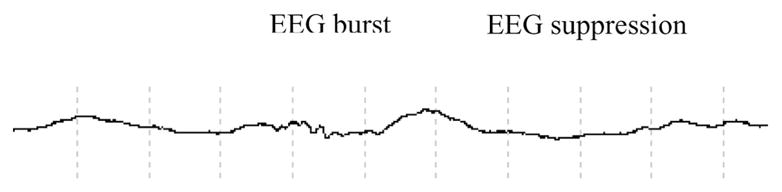
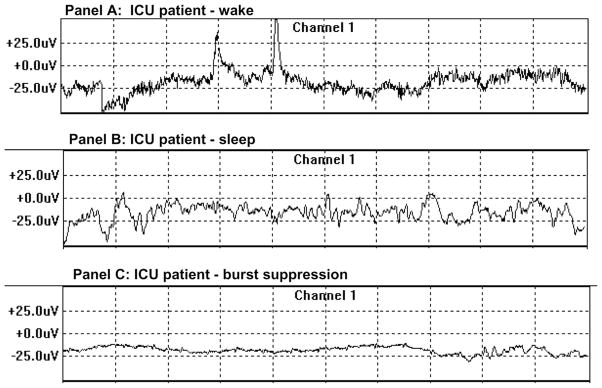
Objectives: This study investigates the possibility of a relationship between oversedation and mortality in mechanically ventilated patients. The presence of burst suppression, a pattern of severely decreased brain wave activity on the electroencephalogram, may be unintentionally induced by heavy doses of sedatives. Burst suppression has never been studied as a potential risk factor for death in patients without a known neurologic disorder or injury.
Design: Post hoc analysis of a prospectively observational cohort study.
Setting: Medical intensive care units of a tertiary care, university-based medical center.
Patients: A total of 125 mechanically ventilated, adult, critically ill patients.
Measurements and main results: A validated arousal scale (Richmond Agitation-Sedation Scale) was used to measure sedation level, and the bispectral index monitor was used to capture electroencephalogram data. Burst suppression occurred in 49 of 125 patients (39%). For analysis, the patients were divided into those with burst suppression (49 of 125, 39%) and those without burst suppression (76 of 125, 61%). All baseline variables were similar between the two groups, with the overall cohort demonstrating a high severity of illness (Acute Physiology and Chronic Health Evaluation II scores of 27.4 +/- 8.2) and 98% receiving sedation. Of those with burst suppression, 29 of 49 (59%) died within 6 months compared with 25 of 76 (33%) who did not demonstrate burst suppression. Using time-dependent Cox regression to adjust for clinically important covariates (age, Charlson comorbidity score, baseline dementia, Acute Physiology and Chronic Health Evaluation II, Sequential Organ Failure Assessment, coma, and delirium), patients who experienced burst suppression were found to have a statistically significant higher 6-month mortality [Hazard's ratio = 2.04, 95% confidence interval, 1.12-3.70, p = 0.02].
Conclusion: The presence of burst suppression, which was unexpectedly high in this medical intensive care unit population, was an independent predictor of increased risk of death at 6 months. This association should be studied prospectively on a larger scale in mechanically ventilated, critically ill patients.
Conflict of interest statement
Drs. Shintani and Tyson have not disclosed any potential conflicts of interest.
Figures
References
-
- Monk TG, Saini V, Weldon BC, et al. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg. 2005;100:4–10. - PubMed
-
- Kress JP, Pohlman AS, O’Connor MF, et al. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471–1477. - PubMed
-
- Kollef MH, Levy NT, Ahrens TS, et al. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114:541–548. - PubMed
-
- Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
