

Comparison of intensity-modulated radiotherapy and forward-planning dynamic arc therapy techniques for prostate cancer
- PMID: 19020481
- PMCID: PMC5722358
- DOI: 10.1120/jacmp.v9i4.2783
Comparison of intensity-modulated radiotherapy and forward-planning dynamic arc therapy techniques for prostate cancer
Abstract
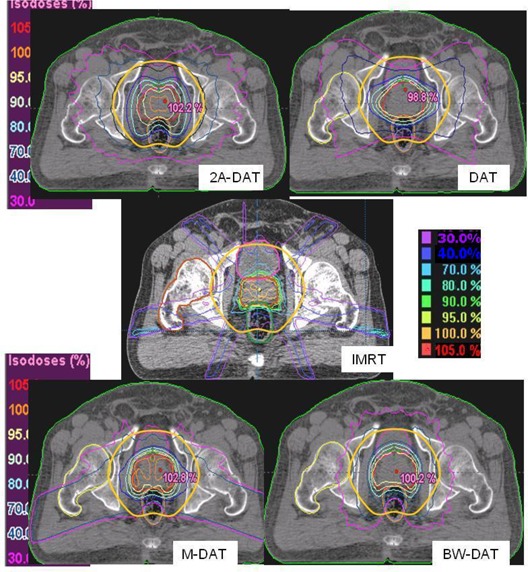
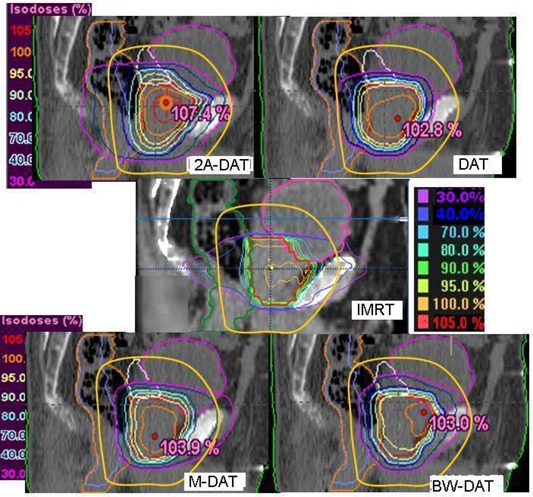
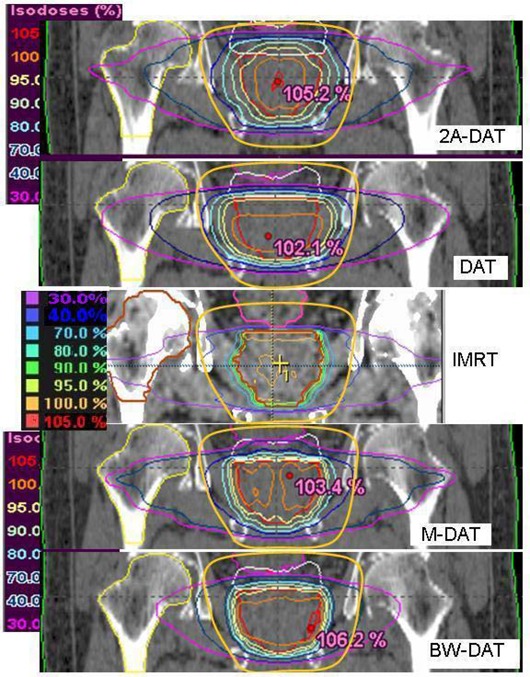
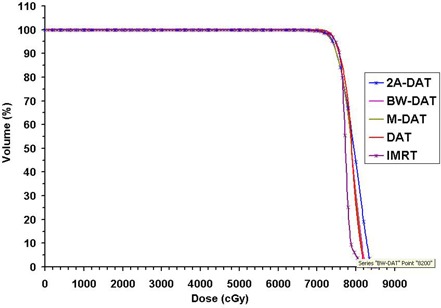
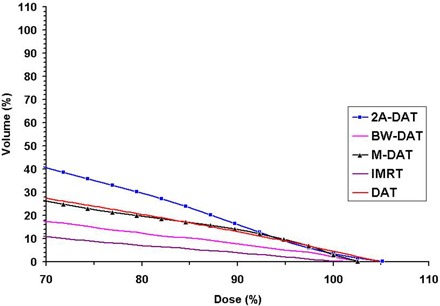
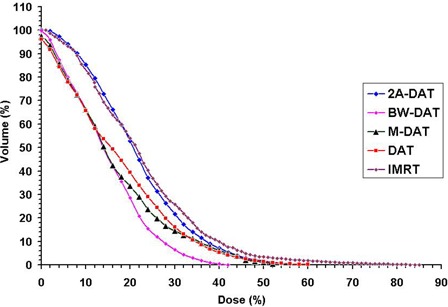
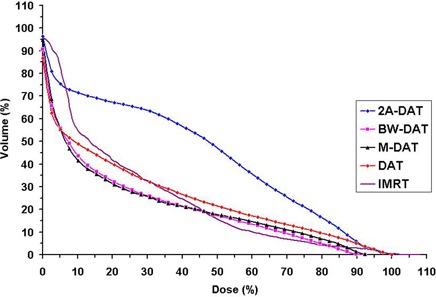
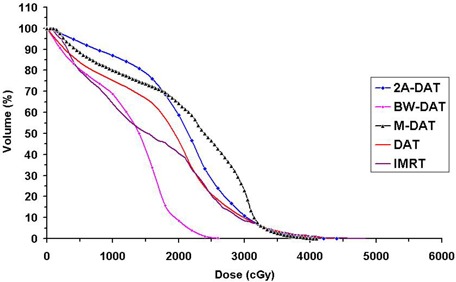
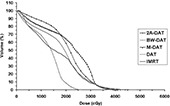
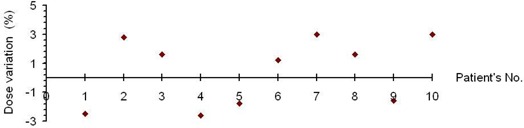
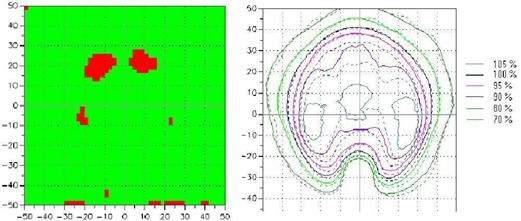
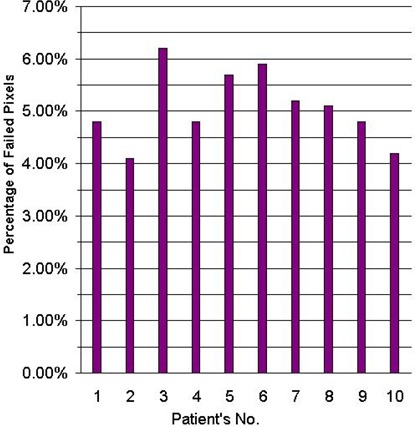
We compare an inverse-planning intensity-modulated radiotherapy (IMRT) technique with three previously published forward-planning dynamic arc therapy techniques and a newly implemented technique for treatment of prostate only. The three previously published dynamic arc techniques are dynamic arc therapy (DAT), two-axis dynamic arc therapy (2A-DAT), and modified dynamic arc therapy (M-DAT). The newly implemented technique is the bilateral wedged dynamic arc (BW-DAT). In all dynamic arcs, the multileaf collimator is moving during rotation to fit the prostate, except that, in 2A-DAT, it is fitting two separate symmetrical rhombi including the prostate. The rectum is shielded during rotation only in the cases of M-DAT and BW-DAT. The results obtained indicate that the BW-DAT, M-DAT, and DAT techniques provide the intended dose coverage of the prescribed dose to the planning target volume (PTV)--that is, 95% of the PTV is covered by 100% of the dose. The maximum dose to a 3-cm margin of healthy tissue that surrounds the PTV is lower by 2.5% in the case of IMRT than in both BW-DAT and M-DAT, but it is lower by 5.0% than that in both DAT and 2A-DAT. The maximum dose to the rest of the healthy tissue in the case of BW-DAT is 33.2 Gy +/- 2.2 Gy. This dose covers percentage healthy body volumes of 8% +/- 3.2% with IMRT, 4% +/- 1.5% with DAT, and 6% +/- 1.2% with both 2A-DAT and M-DAT. Also, this dose is much lower than the accepted maximum dose (52 Gy) to the femoral heads and necks according to Report 62 from the International Commission on Radiation Units and Measurements. Accordingly, it would be possible to neglect delineation of the femoral heads and necks as organs at risk in cases of BW-DAT. Doses to 15%, 25%, 35%, and 50% (D15%, D25%, D35%, and D50%) of the rectum volume in the case of BW-DAT were 43.5 Gy +/- 8.6 Gy, 24.2 Gy +/- 8.7 Gy, 13.2 Gy +/- 4.2 Gy, and 5.7 Gy +/- 2.1 Gy respectively. The D15% of rectum in the case of IMRT was lower than that in BW-DAT, M-DAT, 2A-DAT, and DAT by 7.3%, 10.3%, 33.0%, and 17.6% of the prescribed dose (78 Gy in 39 fractions) respectively. The D25%, D35%, and D50% of the rectum volume in the cases of IMRT and DAT were comparable (with a maximum variation of 4.5%); they were similarly comparable in the cases of M-DAT and BW-DAT (with maximum variation of 1.5%). These same doses in BW-DAT were lower than those in IMRT by 8.7%, 10.6%, and 6.2% respectively, but they were quite lower than those in 2A-DAT, because the average variation was 41.6% (with a maximum of 44.0%). The D15%, D25%, D35%, and D50% of the bladder volume in the case of BW-DAT were 33.2 Gy +/- 10.9 Gy, 17.4 Gy +/- 7.9 Gy, 6.5 Gy +/- 4.3 Gy, and 4.2 Gy +/- 3.5 Gy respectively. The D15% and D25% of the bladder in the cases of IMRT, M-DAT, and BW-DAT were comparable (with a maximum variation of 2.2% and 3.6% respectively), and the mean values of each dose were lower in DAT by 14.3% and 11.7% respectively. However, the values of D35% and D50% in the four techniques were comparable, with maximum variations of 5.1% and 2.7% respectively. The D15%, D25%, D35%, and D50% of the bladder in the case of DAT were lower than those in 2A-DAT by 20.1%, 26.9%, 16.0%, and 2.7% respectively. Ion chamber measurements showed good agreement between the calculated and measured isocentric doses (maximum deviation: 3.2%). Accuracy of the dose distribution calculation for BW-DAT was evaluated by film dosimetry using a gamma index, allowing 3% dose variation and 3 mm distance to agreement as the individual acceptance criteria. We found that fewer than 6.5% of the pixels in the dose distributions of the scanned and calculated area of 10 x 10 cm failed the acceptance criteria. We conclude that, in addition to simplicity of the dose calculation, the BW-DAT technique provides the intended concave dose distribution for treatment of the prostate only. Compared with IMRT, it produces better dose protection to the most of the rectum volume and to the healthy tissue outside the treatment volume. Also, as compared with the other forward planning dynamic arc techniques, it gives the most favorable isodose distributions to the prostate and rectum.
Figures
Similar articles
-
Forward-planning intensity-modulated radiotherapy technique for prostate cancer.J Appl Clin Med Phys. 2007 Nov 5;8(4):114-128. doi: 10.1120/jacmp.v8i4.2488. J Appl Clin Med Phys. 2007. PMID: 18449151 Free PMC article.
-
Stereotactic IMRT for prostate cancer: dosimetric impact of multileaf collimator leaf width in the treatment of prostate cancer with IMRT.J Appl Clin Med Phys. 2004 Spring;5(2):29-41. doi: 10.1120/jacmp.v5i2.1989. Epub 2004 Apr 1. J Appl Clin Med Phys. 2004. PMID: 15738911 Free PMC article. Clinical Trial.
-
Treatment planning and dosimetry of a multi-axis dynamic arc technique for prostate cancer: A comparison with IMRT.Radiat Med. 2006 Jan;24(1):17-22. doi: 10.1007/BF02489984. Radiat Med. 2006. PMID: 16715657
-
Current status of intensity-modulated radiation therapy (IMRT).Int J Clin Oncol. 2007 Dec;12(6):408-15. doi: 10.1007/s10147-007-0703-9. Epub 2007 Dec 21. Int J Clin Oncol. 2007. PMID: 18071859 Review.
-
Recent developments in non-coplanar radiotherapy.Br J Radiol. 2019 May;92(1097):20180908. doi: 10.1259/bjr.20180908. Epub 2019 Feb 1. Br J Radiol. 2019. PMID: 30694086 Free PMC article. Review.
Cited by
-
Beam's-eye-view Dosimetrics-guided inverse planning for aperture-modulated arc therapy.Int J Radiat Oncol Biol Phys. 2009 Dec 1;75(5):1587-95. doi: 10.1016/j.ijrobp.2009.05.003. Epub 2009 Sep 3. Int J Radiat Oncol Biol Phys. 2009. PMID: 19733446 Free PMC article.
-
A dosimetric and treatment efficiency evaluation of stereotactic body radiation therapy for peripheral lung cancer using flattening filter free beams.Oncotarget. 2016 Nov 8;7(45):73792-73799. doi: 10.18632/oncotarget.12071. Oncotarget. 2016. PMID: 27655715 Free PMC article.
References
-
- Lee C, Dong L, Ahamad A, et al. Comparison of treatment volumes and techniques in prostate cancer radiation therapy. Am J Clin Oncol. 2005;28(6):618–625. - PubMed
-
- Zhu S, Mizowaki T, Nagata Y, et al. Comparison of three radiotherapy treatment planning protocols of definitive external‐beam radiation for localized prostate cancer. Int J Clin Oncol. 2005;10(6):398–404. - PubMed
-
- Shiraishi K, Nakagawa K, Yamashita H, Nakamura N, Tago M, Ohtomo K. Treatment planning and dosimetry of a multi‐axis dynamic arc technique for prostate cancer: a comparison with IMRT. Radiat Med. 2006;24(1):17–22. - PubMed
-
- Bauman G, Gete E, Chen J, Wong E. Simplified intensity‐modulated arc therapy for dose escalated prostate cancer radiotherapy. Med Dosim. 2004;29(1):18–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
