

Modeling the association between 43 different clinical and pathological variables and the severity of cognitive impairment in a large autopsy cohort of elderly persons
- PMID: 19021630
- PMCID: PMC2864342
- DOI: 10.1111/j.1750-3639.2008.00244.x
Modeling the association between 43 different clinical and pathological variables and the severity of cognitive impairment in a large autopsy cohort of elderly persons
Abstract
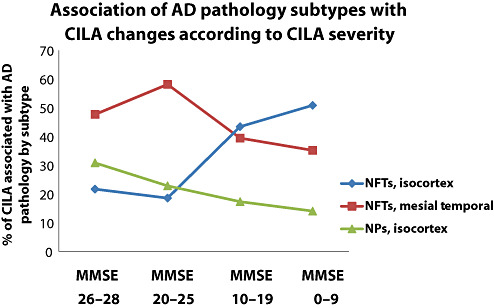
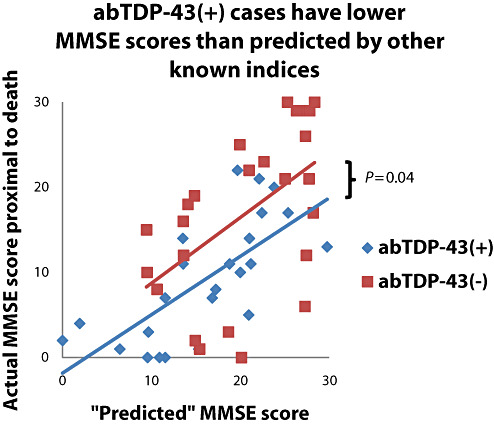
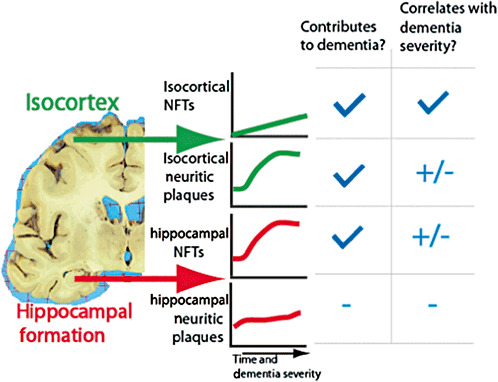
We evaluated the association between mini-mental status examination (MMSE) scores proximal to death and the values of 43 different clinical and pathological parameters. Studies were performed using data from 334 elderly, longitudinally evaluated research subjects who had undergone autopsy and satisfied inclusion criteria from an initial study group of 501. Interindividual variance in MMSE scores was used as a surrogate for the severity of cognitive impairment linked to aging (CILA). A statistical linear regression-based model provided a framework for assessing the parameters with significant, direct impact on CILA severity. Strong association between CILA and Alzheimer's disease (AD) pathology, especially isocortical neurofibrillary tangles, was evident. The pattern of association between AD lesion densities with cognitive impairment severity was biologically informative, with neuritic plaques having more impact in relatively high-functioning individuals. Abundant isocortical Lewy bodies tended to be an additive pathology correlating with final MMSE scores approximately 10 points lower. In a subset of cases we found evidence for association between TDP-43-related pathology and CILA severity, independent of AD or hippocampal sclerosis. There was no support for independent association between CILA severity and most evaluated indices including diffuse plaques, argyrophilic grains, heart disease, education level, apolipoprotein E alleles or diabetes.
Figures


References
-
- Arai T, Hasegawa M, Akiyama H, Ikeda K, Nonaka T, Mori H et al (2006) TDP‐43 is a component of ubiquitin‐positive tau‐negative inclusions in frontotemporal lobar degeneration and amyotrophic lateral sclerosis. Biochem Biophys Res Commun 351:602–611. - PubMed
-
- Armstrong RA (2003) Quantifying the pathology of neurodegenerative disorders: quantitative measurements, sampling strategies and data analysis. Histopathology 42:521–529. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
