

Impact of reperfusion after 3 hours of symptom onset on tissue fate in acute cerebral ischemia
- PMID: 19021836
- PMCID: PMC2755618
- DOI: 10.1111/j.1552-6569.2008.00303.x
Impact of reperfusion after 3 hours of symptom onset on tissue fate in acute cerebral ischemia
Abstract
Background: Reperfusion of penumbral tissue is a promising strategy for treatment of acute cerebral ischemia more than 3 hours from symptom onset. However, there has been only sparse direct evidence that reperfusion after 3 hours prevents infarct growth.
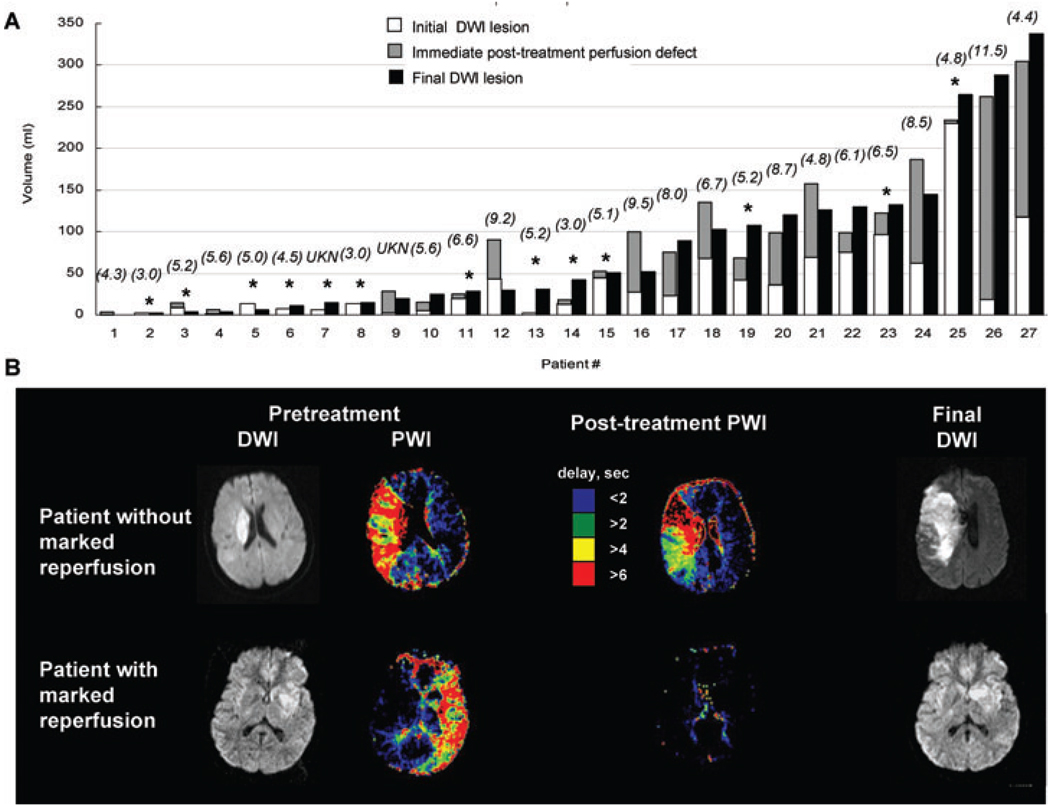
Methods: We analyzed clinical and serial magnetic resonance imaging (MRI) data on patients who received endovascular recanalization therapy 3-12 hours after last known well time. Multimodal MRIs were acquired pretreatment, early (1-20 hours), and late (2-7 days) after treatment. Degree of recanalization was assessed on end of procedure catheter angiogram, degree of reperfusion on early posttreatment perfusion MRI, and infarct growth by analysis of diffusion lesion volumes on pretreatment and late MRIs.
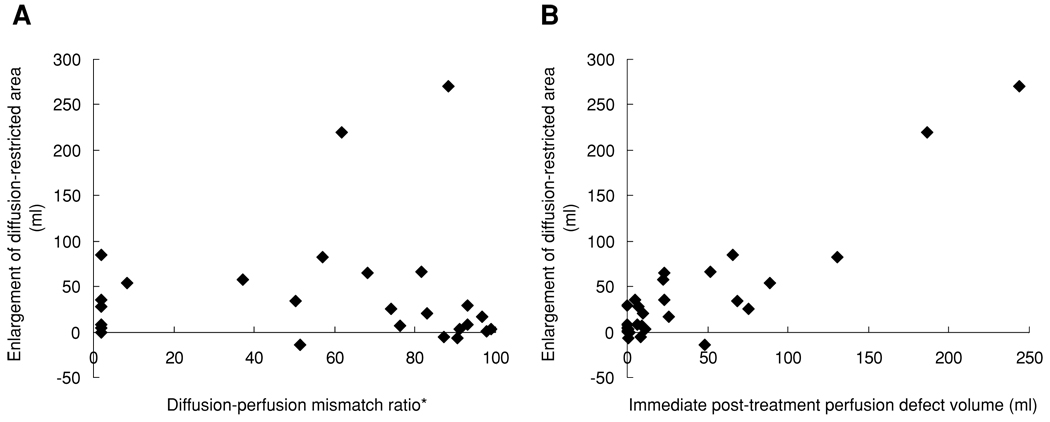
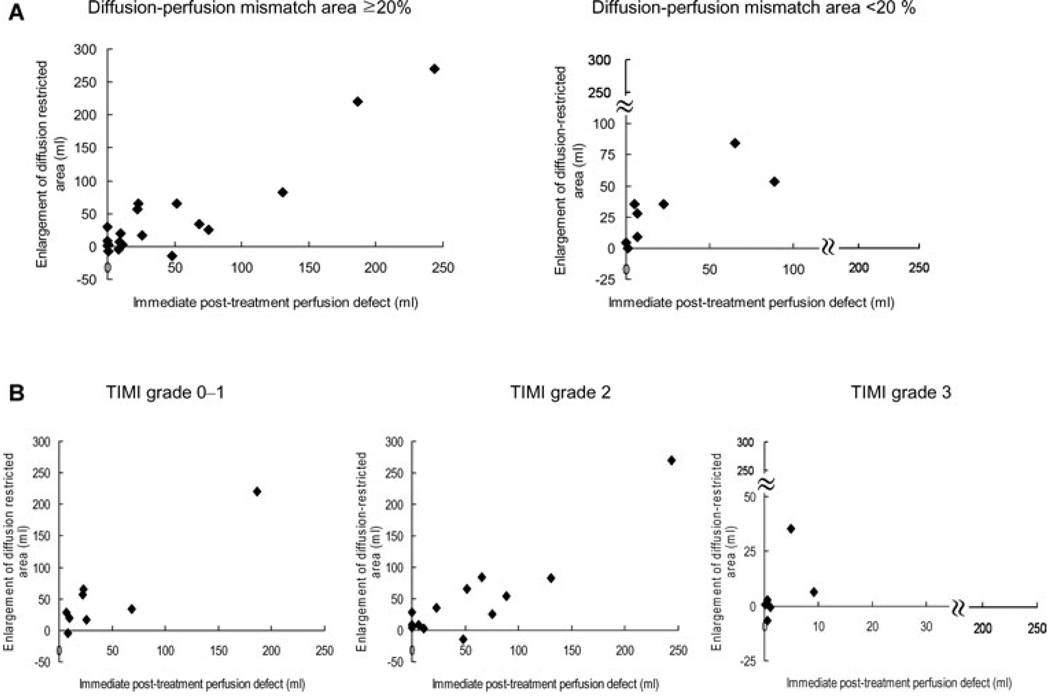
Results: Twenty-seven (12 men, 15 women) underwent endovascular recanalization procedures at 6.0 +/- 2.1 hours (range, 3.0-11.5 hours) after last known well time. Immediate posttreatment perfusion lesion (Tmax > or =4 seconds) volume correlated strongly with infarct growth (r= .951, P < .001), exceeding the correlations of vessel recanalization score (r=-.198, P= .446) and pretreatment diffusion-perfusion mismatch volume (r= .518, P= .033). Without reperfusion, enlargement of DWI lesion volume was observed in all patients, and extent of enlargement depended on volume of immediate posttreatment perfusion defects.
Conclusion: Our data indicate that posttreatment reperfusion is the major determinant of threatened tissue outcome, and suggest reperfusion even after 3 hours of symptom onset can alter tissue fate over a wide range of mismatch volumes.
Figures
References
-
- Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of atlantis, ecass, and ninds rt-pa stroke trials. Lancet. 2004;363:768–774. - PubMed
-
- Rother J, Schellinger PD, Gass A, et al. Effect of intravenous thrombolysis on MRI parameters and functional outcome in acute stroke <6 hours. Stroke. 2002;33:2438–2445. - PubMed
-
- Parsons MW, Barber PA, Chalk J, et al. Diffusion- and perfusion-weighted MRI response to thrombolysis in stroke. Ann Neurol. 2002;51:28–37. - PubMed
-
- Schellinger PD, Fiebach JB, Jansen O, et al. Stroke magnetic resonance imaging within 6 hours after onset of hyperacute cerebral ischemia. Ann Neurol. 2001;49:460–469. - PubMed
-
- Hjort N, Butcher K, Davis SM, et al. Magnetic resonance imaging criteria for thrombolysis in acute cerebral infarct. Stroke. 2005;36:388–397. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
