

End-expiratory lung volume during mechanical ventilation: a comparison with reference values and the effect of positive end-expiratory pressure in intensive care unit patients with different lung conditions
- PMID: 19021898
- PMCID: PMC2646307
- DOI: 10.1186/cc7125
End-expiratory lung volume during mechanical ventilation: a comparison with reference values and the effect of positive end-expiratory pressure in intensive care unit patients with different lung conditions
Erratum in
- Crit Care. 2009;13(6):430
Abstract
Introduction: Functional residual capacity (FRC) reference values are obtained from spontaneous breathing patients, and are measured in the sitting or standing position. During mechanical ventilation FRC is determined by the level of positive end-expiratory pressure (PEEP), and it is therefore better to speak of end-expiratory lung volume. Application of higher levels of PEEP leads to increased end-expiratory lung volume as a result of recruitment or further distention of already ventilated alveoli. The aim of this study was to measure end-expiratory lung volume in mechanically ventilated intensive care unit (ICU) patients with different types of lung pathology at different PEEP levels, and to compare them with predicted sitting FRC values, arterial oxygenation, and compliance values.
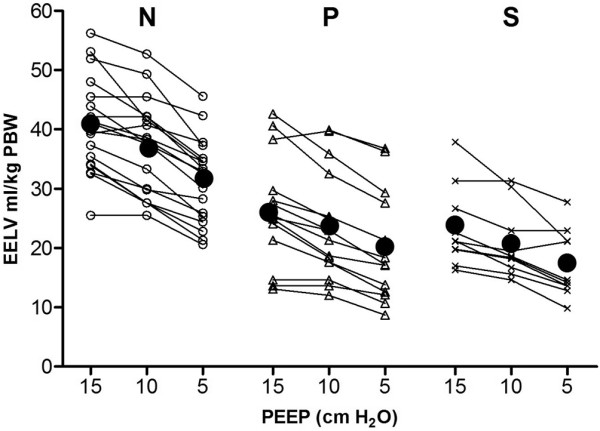
Methods: End-expiratory lung volume measurements were performed at PEEP levels reduced sequentially (15, 10 and then 5 cmH2O) in 45 mechanically ventilated patients divided into three groups according to pulmonary condition: normal lungs (group N), primary lung disorder (group P), and secondary lung disorder (group S).
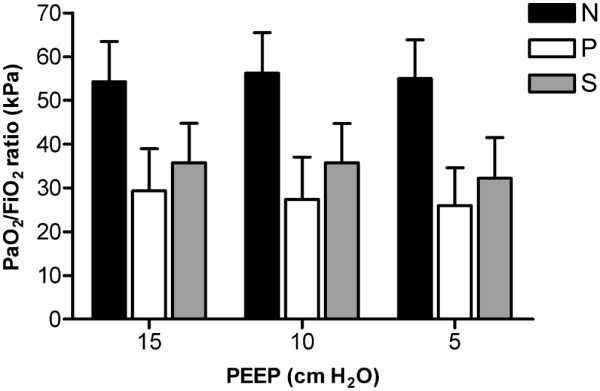
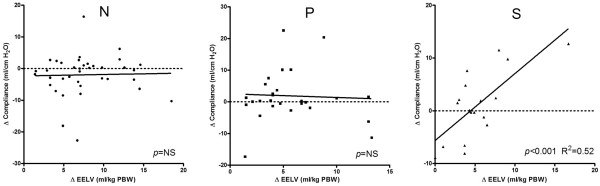
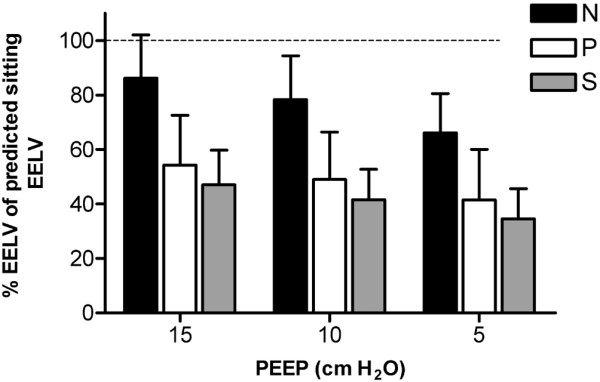
Results: In all three groups, end-expiratory lung volume decreased significantly (P < 0.001) while PEEP decreased from 15 to 5 cmH2O, whereas the ratio of arterial oxygen tension to inspired oxygen fraction did not change. At 5 cmH2O PEEP, end-expiratory lung volume was 31, 20, and 17 ml/kg predicted body weight in groups N, P, and S, respectively. These measured values were only 66%, 42%, and 34% of the predicted sitting FRC. A correlation between change in end-expiratory lung volume and change in dynamic compliance was found in group S (P < 0.001; R2 = 0.52), but not in the other groups.
Conclusions: End-expiratory lung volume measured at 5 cmH2O PEEP was markedly lower than predicted sitting FRC values in all groups. Only in patients with secondary lung disorders were PEEP-induced changes in end-expiratory lung volume the result of derecruitment. In combination with compliance, end-expiratory lung volume can provide additional information to optimize the ventilator settings.
Figures
References
-
- Drummond GB. Computed tomography and pulmonary measurements. Br J Anaesth. 1998;80:665–671. - PubMed
-
- Gattinoni L, Caironi P, Pelosi P, Goodman LR. What has computed tomography taught us about the acute respiratory distress syndrome? Am J Respir Crit Care Med. 2001;164:1701–1711. - PubMed
-
- East TD, Wortelboer PJ, van Ark E, Bloem FH, Peng L, Pace NL, Crapo RO, Drews D, Clemmer TP. Automated sulfur hexafluoride washout functional residual capacity measurement system for any mode of mechanical ventilation as well as spontaneous respiration. Crit Care Med. 1990;18:84–91. doi: 10.1097/00003246-199001000-00018. - DOI - PubMed
-
- Di Marco F, Rota SL, Milan B, Stucchi R, Centanni S, Brochard L, Fumagalli R. Measurement of functional residual capacity by helium dilution during partial support ventilation: in vitro accuracy and in vivo precision of the method. Intensive Care Med. 2007;33:2109–2115. doi: 10.1007/s00134-007-0833-6. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
