

Connection of discontinuous pulmonary arteries in patients with a superior or total cavopulmonary circulation
- PMID: 19022015
- PMCID: PMC4227614
- DOI: 10.1016/j.athoracsur.2008.07.072
Connection of discontinuous pulmonary arteries in patients with a superior or total cavopulmonary circulation
Abstract
Background: Discontinuous pulmonary arteries (PAs) may develop in patients with single-ventricle heart disease from a variety of causes. We investigated factors associated with successful connection of nonconfluent PAs in patients with a cavopulmonary circulation.
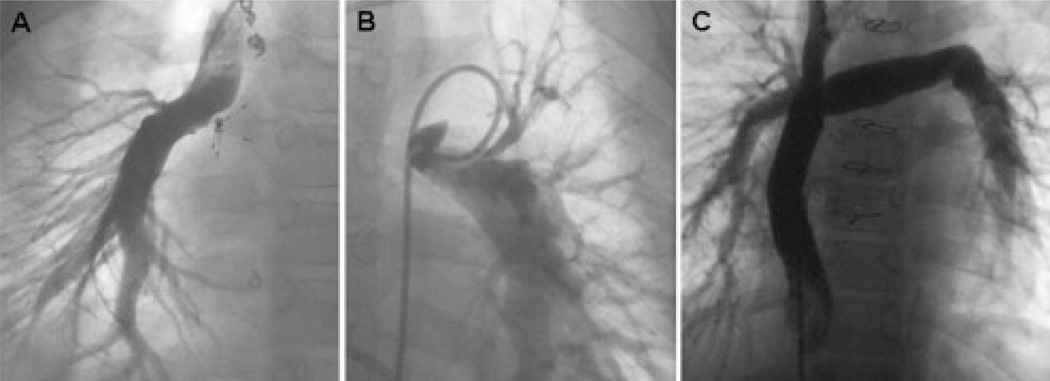
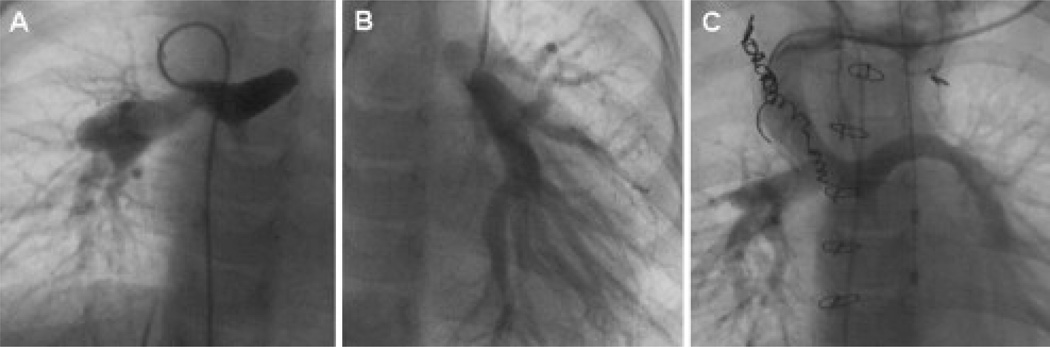
Methods: We reviewed 49 patients who underwent connection of discontinuous PAs with or after a bidirectional Glenn (n = 29) or Fontan (n = 20) procedure at a median age of 7.9 years. PA continuity was established by direct anastomosis in 27, interposition graft in 19, and transcatheter recanalization in 3. Survival was 92% +/- 4% at 1 year and 89% +/- 5% at 5 years.
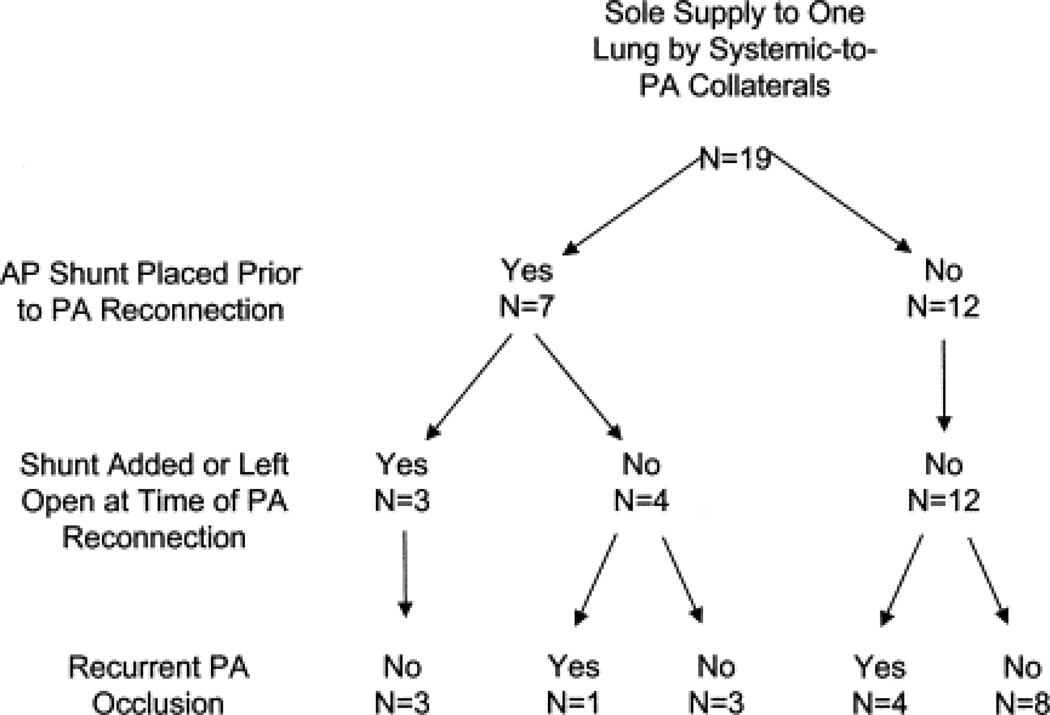
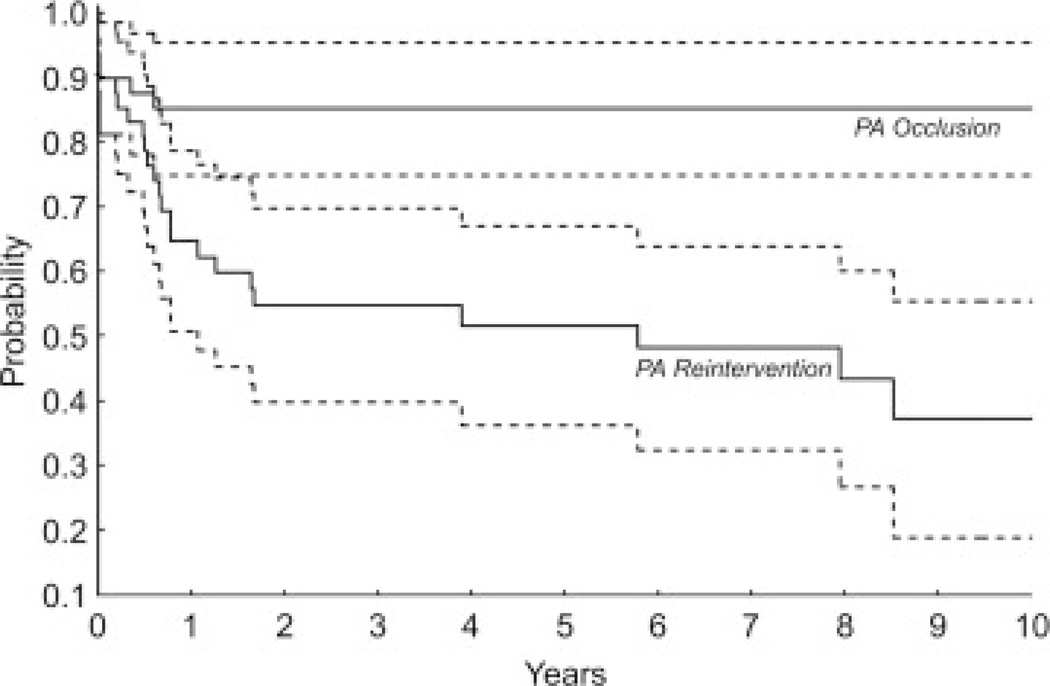
Results: Recurrent PA occlusion was documented in 7 patients, 5 within 10 days of PA connection. The only factor associated with shorter freedom from PA occlusion was sole supply of blood flow to 1 lung by systemic-to-PA collaterals before connection (66% +/- 14% vs 95% +/- 4% freedom from occlusion at 6 months, p = 0.03). Among the 45 early survivors, freedom from PA reintervention or occlusion was 83 +/- 6% at 1 year and 55 +/- 9% at 3 years.
Conclusions: Discontinuous PAs can be successfully connected in most patients with a cavopulmonary circulation, although nonconfluent PAs appear to increase the risk of poor outcome after Fontan. Recurrent PA occlusion was usually diagnosed in the early postoperative period. In patients with sole supply to 1 lung through collaterals, shunt placement before PA connection may optimize outcome. A low threshold for investigation of the reconnected PA is warranted.
Figures
References
-
- Choussat, Fontan F, Besse P, Vallot F, Chauve A, Bricaud H. Selection criteria for Fontan's procedure. In: Anderson RH, Shinebourne EA, editors. Paediatric cardiology 1977. Edinburgh: Churchill Livingstone; 1978. pp. 559–566.
-
- Gentles TL, Mayer JE, Jr, Gauvreau K, et al. Fontan operation in five hundred consecutive patients: factors influencing early and late outcome. J Thorac Cardiovasc Surg. 1997;114:376–391. - PubMed
-
- Fontan F, Fernandez G, Costa F, et al. The size of the pulmonary arteries and the results of the Fontan operation. J Thorac Cardiovasc Surg. 1989;98:711–719. - PubMed
-
- Knott-Craig CJ, Julsrud PR, Schaff HV, Puga FJ, Danielson GK. Pulmonary artery size and clinical outcome after the modified Fontan operation. Ann Thorac Surg. 1993;55:646–651. - PubMed
-
- Senzaki H, Isoda T, Ishizawa A, Hishi T. Reconsideration of criteria for the Fontan operation: Influence of pulmonary artery size on postoperative hemodynamics of the Fontan operation. Circulation. 1994;89:266–271. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
