

Do normal radiographs exclude asphericity of the femoral head-neck junction?
- PMID: 19023635
- PMCID: PMC2635443
- DOI: 10.1007/s11999-008-0617-5
Do normal radiographs exclude asphericity of the femoral head-neck junction?
Abstract
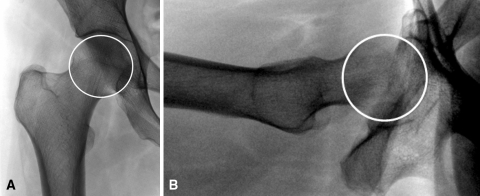
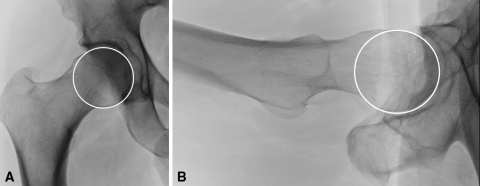
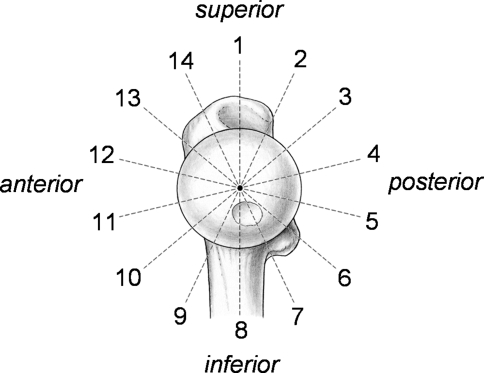
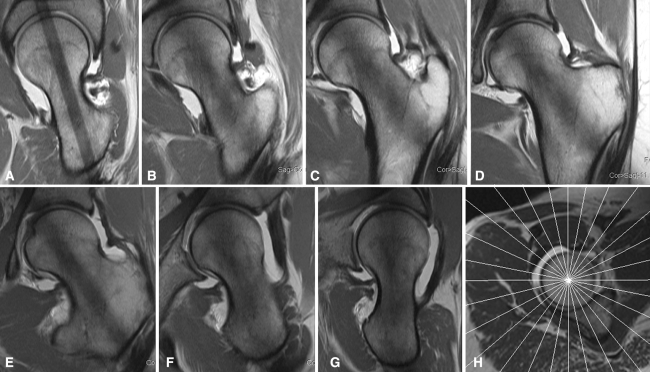
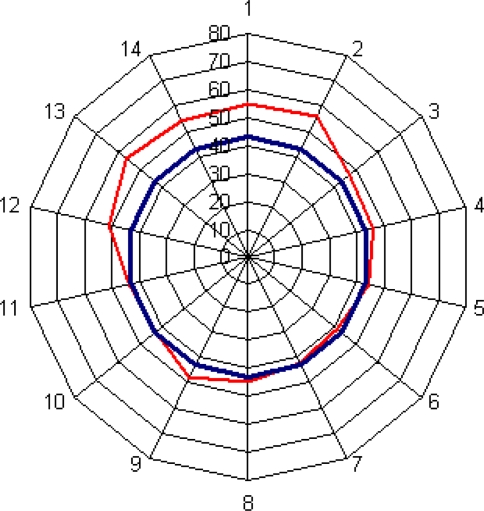
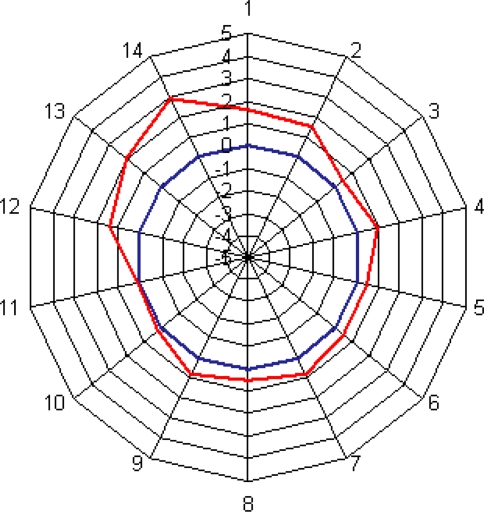
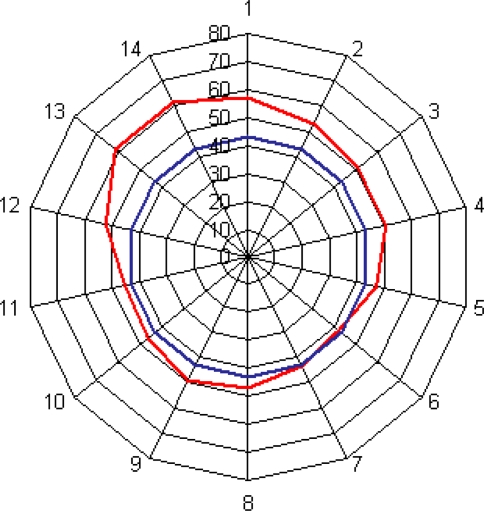
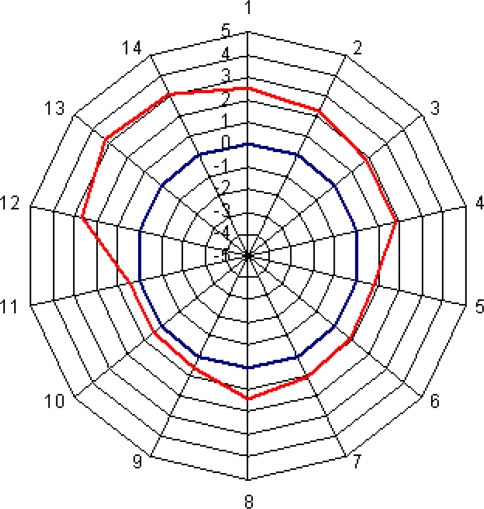
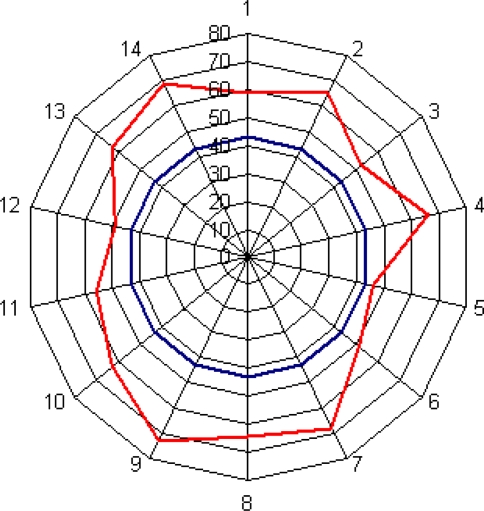
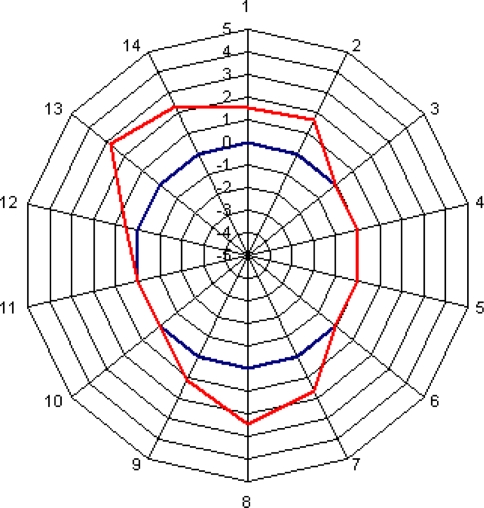
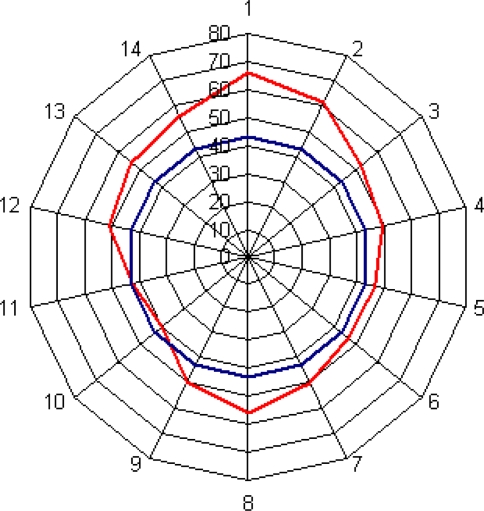
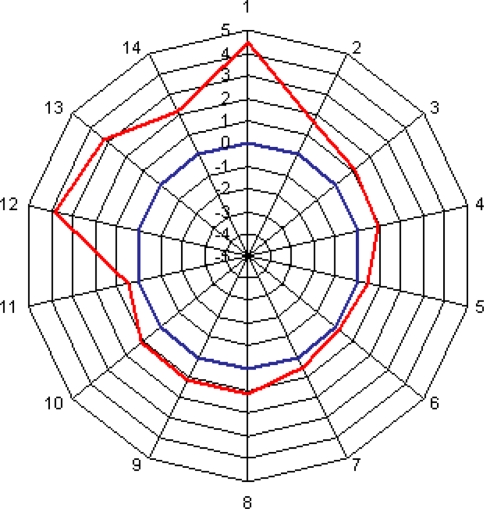
Asphericity of the femoral head-neck junction is one cause for femoroacetabular impingement of the hip. However, the asphericity often is underestimated on conventional radiographs. This study compares the presence of asphericity on conventional radiographs with its appearance on radial slices of magnetic resonance arthrography (MRA). We retrospectively reviewed 58 selected hips in 148 patients who underwent a surgical dislocation of the hip. To assess the circumference of the proximal femur, alpha angle and height of asphericity were measured in 14 positions using radial slices of MRA. The hips were assigned to one of four groups depending on the appearance of the head-neck junction on anteroposterior pelvic and lateral crosstable radiographs. Group I (n = 19) was circular on both planes, Group II (n = 19) was aspheric on the crosstable view, Group III (n = 4) was aspheric on the anteroposterior view, and Group IV (n = 13) was aspheric on both views. In all four groups, the highest alpha angle was found in the anterosuperior area of the head-neck junction. Even when conventional radiographs appeared normal, an increased alpha angle was present anterosuperiorly. Without the use of radial slices in MRA, the asphericity would be underestimated in these patients.
Figures


References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '15921872', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15921872/'}]}
- Beaule PE, Zaragoza E, Motamedi K, Copelan N, Dorey FJ. Three-dimensional computed tomography of the hip in the assessment of femoroacetabular impingement. J Orthop Res. 2005;23:1286–1292. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1302/0301-620X.87B7.15203', 'is_inner': False, 'url': 'https://doi.org/10.1302/0301-620x.87b7.15203'}, {'type': 'PubMed', 'value': '15972923', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15972923/'}]}
- Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012–1018. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/BLO.0b013e3180f60b53', 'is_inner': False, 'url': 'https://doi.org/10.1097/blo.0b013e3180f60b53'}, {'type': 'PubMed', 'value': '17589367', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17589367/'}]}
- Clohisy JC, Nunley RM, Otto RJ, Schoenecker PL. The frog-leg lateral radiograph accurately visualized hip cam impingement abnormalities. Clin Orthop Relat Res. 2007;462:115–121. - PubMed
-
- None
- Eijer H, Leunig M, Mahomed M, Ganz R. Crosstable lateral radiograph for screening of anterior femoral head-neck offset in patients with femoroacetabular impingement. Hip Int. 2001;11:37–41.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1302/0301-620X.83B8.11964', 'is_inner': False, 'url': 'https://doi.org/10.1302/0301-620x.83b8.11964'}, {'type': 'PubMed', 'value': '11764423', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11764423/'}]}
- Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83:1119–1124. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
