

The epidemiology and medical management of low back pain during ambulatory medical care visits in the United States
- PMID: 19025636
- PMCID: PMC2631527
- DOI: 10.1186/1750-4732-2-11
The epidemiology and medical management of low back pain during ambulatory medical care visits in the United States
Abstract
Background: Low back pain (LBP) is a common symptom.
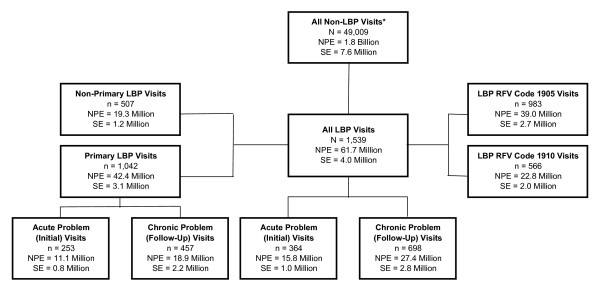
Methods: Patient visits attributed to LBP in the National Ambulatory Medical Care Survey (NAMCS) during 2003-2004 served as the basis for epidemiological analyses (n = 1539). The subset of patient visits in which LBP was the primary reason for seeking care (primary LBP patient visits) served as the basis for medical management analyses (n = 1042). National population estimates were derived using statistical weighting techniques.
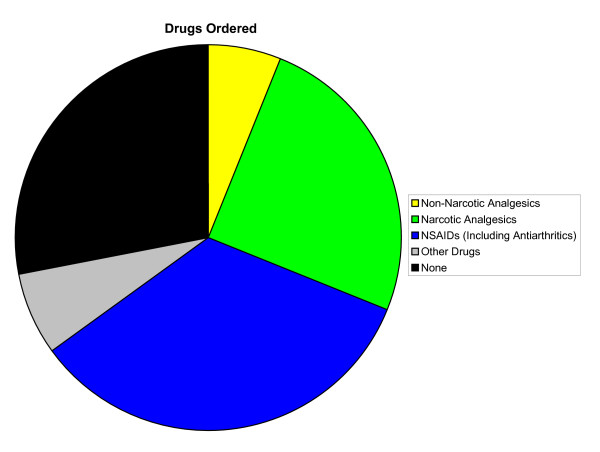
Results: There were 61.7 million (SE, 4.0 million) LBP patient visits and 42.4 million (SE, 3.1 million) primary LBP patient visits. Only 55% of LBP patient visits were provided by primary care physicians. Age, geographic region, chronicity of symptoms, injury, type of physician provider, and physician specialty were associated with LBP patient visits. Age, injury, primary care physician status, type of physician provider, and shared physician care were associated with chronicity of LBP care. Osteopathic physicians were more likely than allopathic physicians to provide medical care during LBP patient visits (odds ratio [OR], 2.61; 95% confidence interval [CI], 1.75-3.92) and chronic LBP patient visits (OR, 4.39; 95% CI, 2.47-7.80). Nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotic analgesics were ordered during 14.2 million (SE, 1.2 million) and 10.5 million (SE, 1.1 million) primary LBP patient visits, respectively. Drugs (OR, 0.29; 95% CI, 0.13-0.62) and, specifically, NSAIDs (OR, 0.40; 95% CI, 0.25-0.64) were ordered less often during chronic LBP patient visits compared with acute LBP patient visits. Overall, osteopathic physicians were less likely than allopathic physicians to order NSAIDs for LBP (OR, 0.43; 95% CI, 0.24-0.76). Almost two million surgical procedures were ordered, scheduled, or performed during primary LBP patient visits.
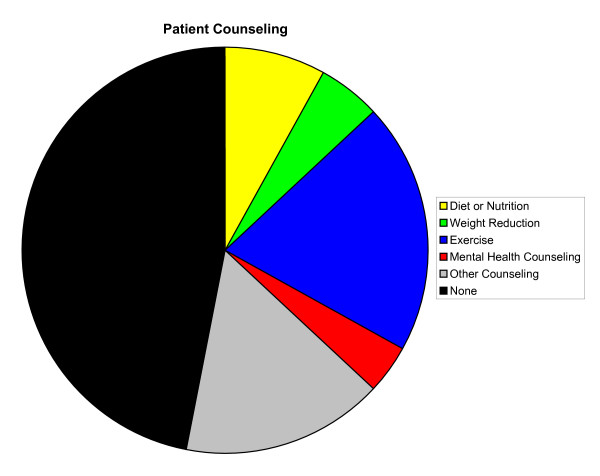
Conclusion: The percentage of LBP visits provided by primary care physicians in the United States remains suboptimal. Medical management of LBP, particularly chronic LBP, appears to over-utilize surgery relative to more conservative measures such as patient counseling, non-narcotic analgesics, and other drug therapies. Osteopathic physicians are more likely to provide LBP care, and less likely to use NSAIDs during such visits, than their allopathic counterparts. In general, LBP medical management does not appear to be in accord with evidence-based guidelines.
Figures
References
-
- Hanchak NA, Murray JF, Hirsch A, McDermott PD, Schlackman N. USQA health profile database as a tool for health plan quality improvement. Manag Care Q. 1996;4:58–69. - PubMed
-
- Bigos SJ, Bowyer OR, G Braen GR, Brown K, Deyo R, Haldeman S, Hart JL, Johnson EW, Keller R, Kido D, Liang MH, Nelson RM, Nordin M, Owen BD, Pope MH, Schwartz RK, Stewart DH, Susman J, Triano JJ, Tripp LC, Turk DC, Watts C, Weinstein JN. Acute Low Back Problems in Adults. Clinical Practice Guideline No. 14. Rockville, MD: Agency for Healthcare Research and Quality, Public Health Service, U.S. Department of Health and Human Services; 1994.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
