

Harmonic scalpel versus electrocautery for harvest of radial artery conduits: reduced risk of spasm and intimal injury on optical coherence tomography
- PMID: 19026820
- PMCID: PMC2649709
- DOI: 10.1016/j.jtcvs.2008.05.060
Harmonic scalpel versus electrocautery for harvest of radial artery conduits: reduced risk of spasm and intimal injury on optical coherence tomography
Abstract
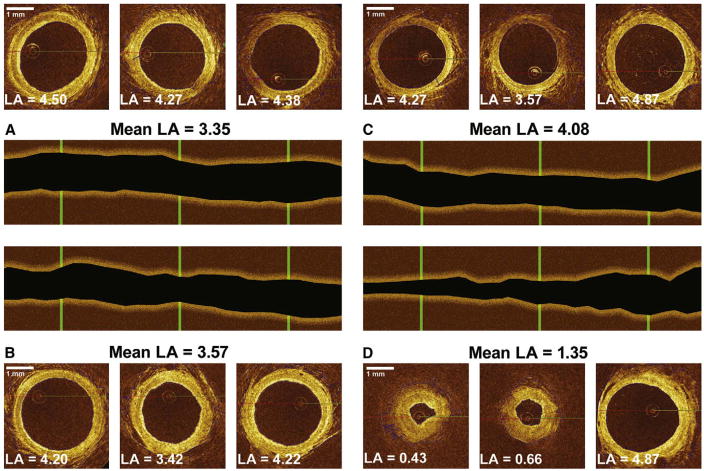
Objective: Vasospasm is the primary obstacle to widespread adoption of the radial artery as a conduit in coronary artery bypass grafting. We used optical coherence tomography, a catheter-based intravascular imaging modality, to measure the degree of radial artery spasm induced by means of harvest with electrocautery or a harmonic scalpel in patients undergoing coronary artery bypass grafting.
Methods: Radial arteries were harvested from 44 consecutive patients with a harmonic scalpel (n = 15) or electrocautery (n = 29). Vessels were imaged before harvesting and after removal from the arm, with saphenous vein tracts serving as internal controls. Optical coherence tomographic findings for the degree of harvesting-induced injury were validated against histologic measures.
Results: Optical coherence tomographic measures of endovascular dimensions and injury correlated strongly with histologic findings. Mean luminal volume, a measure of vasospasm, decreased significantly less after harvesting with a harmonic scalpel (9% +/- 7%) than with electrocautery (35% +/- 6%, P = .015). Completely intact intima was present in 11 (73%) of 15 radial arteries harvested with a harmonic scalpel (73%) compared with 9 of 29 arteries harvested by means of electrocautery (31%, P = .011). Intraoperative flow measurements and patency rates at 5 days postoperatively were not significantly different among groups.
Conclusions: Optical coherence tomography provides a level of speed and accuracy for quantifying endothelial injury and vasospasm that has not been described for any other modality, suggesting potential as an intraoperative quality assurance tool. Our optical coherence tomographic findings suggest that the harmonic scalpel induces less spasm and intimal injury compared with electrocautery.
Figures


References
-
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery) ACC/AHA 2004 guideline update for coronary artery bypass graft surgery. Circulation. 2004;110:e340–437. (erratum appears in Circulation. 2005;111:2014) - PubMed
-
- Desai ND, Cohen EA, Naylor CD, Fremes SE for the Radial Artery Patency Study Investigators. A randomized comparison of radial-artery and saphenous-vein coronary bypass grafts. N Engl J Med. 2004;351:2302–9. - PubMed
-
- Miwa S, Desai N, Koyama T, et al. Radial artery angiographic string sign: clinical consequences and the role of pharmacologic therapy. Ann Thorac Surg. 2006;81:112–8. - PubMed
-
- Chong CF, Moat NE, Collins P. Radial artery grafts’ string-sign—role of graft spasm and competitive flow. Interact Cardiovasc Thorac Surg. Epub September 15, 2006.
-
- Desai ND, Naylor CD, Kiss A, et al. Impact of patient and target-vessel characteristics on arterial and venous bypass graft patency: insight from a randomized trial. Circulation. 2007;115:684–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
