

Epidemiology of sudden cardiac death: clinical and research implications
- PMID: 19026856
- PMCID: PMC2621010
- DOI: 10.1016/j.pcad.2008.06.003
Epidemiology of sudden cardiac death: clinical and research implications
Abstract
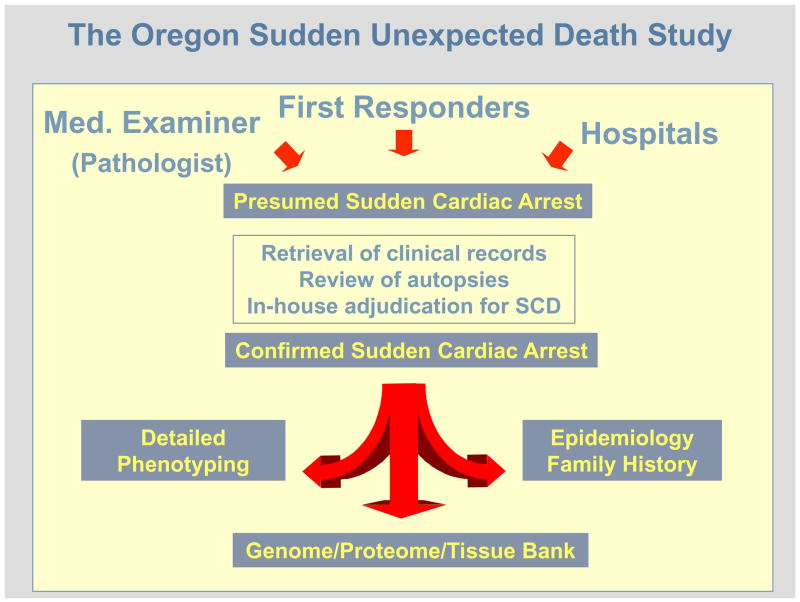
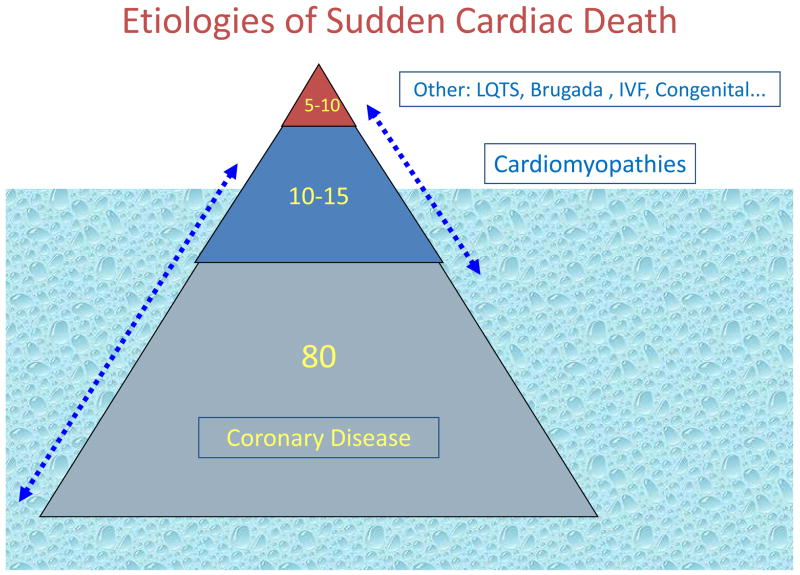
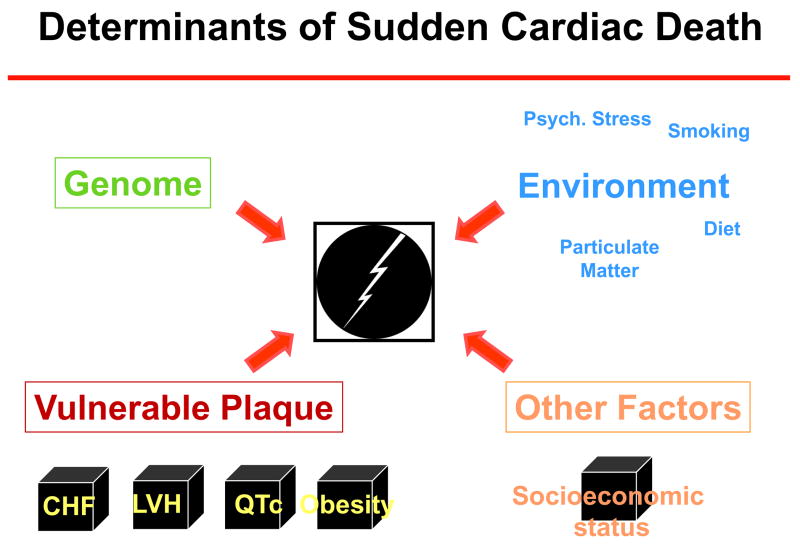
The current annual incidence of sudden cardiac death in the United States is likely to be in the range of 180,000 to 250,000 per year. Coinciding with the decreased mortality from coronary artery disease, there is evidence pointing toward a significant decrease in rates of sudden cardiac death in the United States during the second half of the 20th century. However, the alarming rise in prevalence of obesity and diabetes in the first decade of the new millennium both in the United States and worldwide, would indicate that this favorable trend is unlikely to persist. We are likely to witness a resurgence of coronary artery disease and heart failure, as a result of which sudden cardiac death will have to be confronted as a shared and indiscriminate, worldwide public health problem. There is also increasing recognition of the fact that discovery of meaningful and relevant risk stratification and prevention methodologies will require careful prospective community-wide analyses, with access to large archives of DNA, serum, and tissue that link with well-phenotyped databases. The purpose of this review is to summarize current knowledge of sudden cardiac death epidemiology. We will discuss the significance and strengths of community-wide evaluations of sudden cardiac death, summarize recent observations from such studies, and finally highlight specific potential predictors that warrant further evaluation as determinants of sudden cardiac death in the general population.
Figures
Comment in
-
Cardiopulmonary resuscitation: is the ED visit an opportunity to recommend education?Am J Emerg Med. 2013 Feb;31(2):426-8. doi: 10.1016/j.ajem.2012.09.028. Epub 2012 Nov 15. Am J Emerg Med. 2013. PMID: 23159428 No abstract available.
References
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349(9064):1498–504. - PubMed
-
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349(9063):1436–42. - PubMed
-
- Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997;349(9061):1269–76. - PubMed
-
- Okrainec K, Banerjee DK, Eisenberg MJ. Coronary artery disease in the developing world. Am Heart J. 2004;148(1):7–15. - PubMed
-
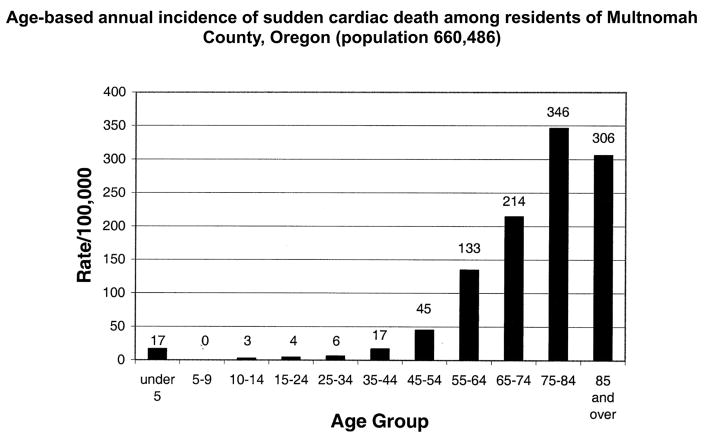
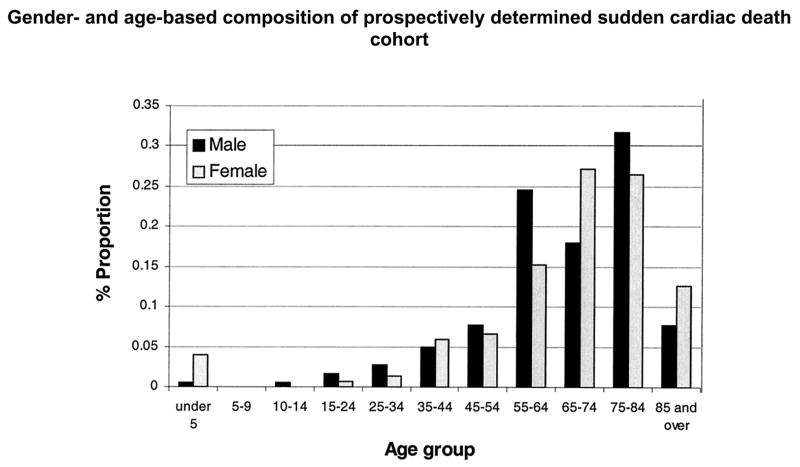
- Chugh SS, Jui J, Gunson K, Stecker EC, John BT, Thompson B, Ilias N, Vickers C, Dogra V, Daya M, Kron J, Zheng ZJ, Mensah G, McAnulty J. Current burden of sudden cardiac death: multiple source surveillance versus retrospective death certificate-based review in a large U.S. community. J Am Coll Cardiol. 2004;44(6):1268–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
