

CD146(+) bone marrow osteoprogenitors increase in the advanced stages of primary myelofibrosis
- PMID: 19029148
- PMCID: PMC2625423
- DOI: 10.3324/haematol.13598
CD146(+) bone marrow osteoprogenitors increase in the advanced stages of primary myelofibrosis
Abstract
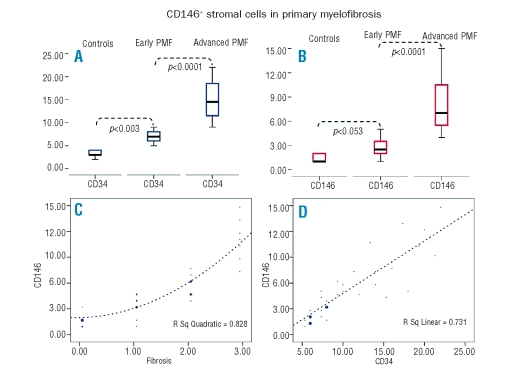
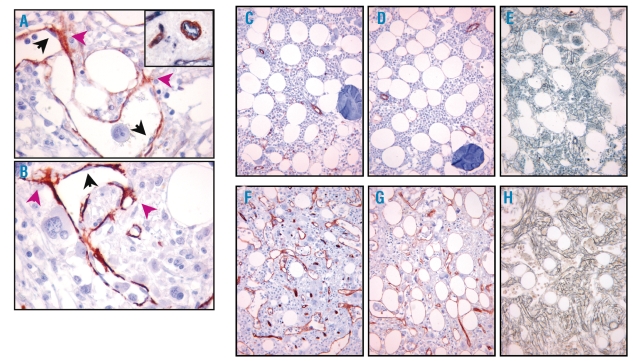
CD146(+) bone marrow stromal cells have been recently recognized as clonogenic osteoprogenitors able to organize a complete hematopoietic microenvironment. In this study we used immunohistochemical analysis to investigate the contribution of CD146(+) bone marrow osteoprogenitors to the stromal remodeling occurring in the different stages of primary myelofibrosis. We found that CD146(+) cells sited at the abluminal side of the bone marrow vessels and branching among hematopoietic cells significantly increased in the advanced stages of primary myelofibrosis (p<0.001), paralleling the extent of fibrosis (rho=0.916, p<0.0001) and the microvascular density (r=0.883, p<0.0001). Coherently with a mural cell function, such cells also displayed smooth-muscle actin expression. Our data providing evidence of CD146(+) cell involvement in bone marrow stromal changes occurring in primary myelofibrosis are consistent with the capability of these cells to participate in fiber deposition, angiogenesis, and bone formation. They could also represent rationale for new therapies targeting the bone marrow stroma in primary myelofibrosis.
Figures
References
-
- Tefferi A, Vardiman JW. Classification and diagnosis of myeloproliferative neoplasms: the 2008 World Health Organization criteria and point-of-care diagnostic algorithms. Leukemia. 2008;22:14–22. - PubMed
-
- Thiele J, Kvasnicka HM. Hemato-pathologic findings in chronic idiopathic myelofibrosis. Semin Oncol. 2005;32:380–94. - PubMed
-
- Mesa RA, Hanson Ca, Rajkumar V, Schroeder G, Tefferi A. Evaluation and clinical correlations of bone marrow angiogenesis in myelofibrosis with myeloid metaplasia. Blood. 2000;96:3374–80. - PubMed
-
- Boveri E, Passamonti F, Rumi E, Pietra D, Elena C, Arcaini L, et al. Bone marrow microvessel density in chronic myeloproliferative disorders: a study of 115 patients with clinicopathological and molecular corelations. Br J Haematol. 2007;140:162–8. - PubMed
-
- Vener C, Fracchiolla NS, Gianelli U, Calori R, Radaelli F, Iurlo A, et al. Prognostic implications of the European consensus for grading of bone marrow fibrosis in chronic idiopathic myelofibrosis. Blood. 2008;111:1862–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
