

Percutaneous core excision and radiofrequency thermo-coagulation for the ablation of osteoid osteoma of the spine
- PMID: 19031087
- PMCID: PMC2899413
- DOI: 10.1007/s00586-008-0791-x
Percutaneous core excision and radiofrequency thermo-coagulation for the ablation of osteoid osteoma of the spine
Abstract
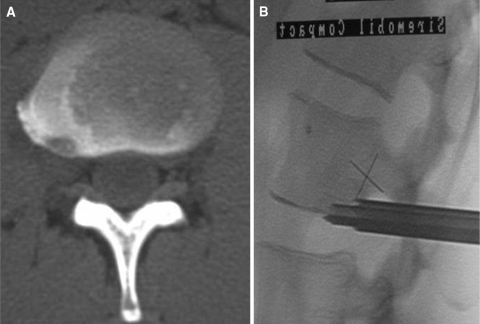
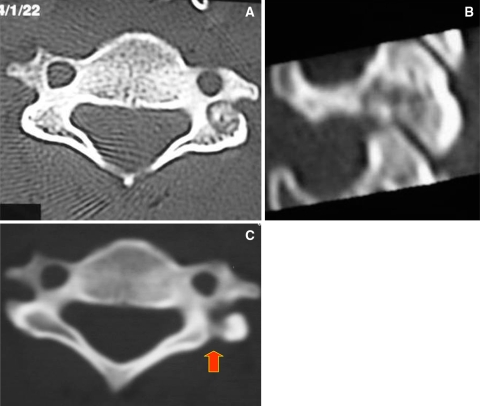
Percutaneous radiofrequency ablation is the treatment of choice for osteoid osteoma of the appendicular skeleton. However, difficulties in localizing the lesion in the spine and its proximity to neural elements have yet to make it the prevalent treatment for spine. This study assesses the safety and effectiveness of two percutaneous techniques for ablating osteoid osteoma of the spine. Seven patients were treated between 1998 and 2005. Four patients underwent percutaneous radiofrequency coagulation. The lesions were located at the articular processes of L3 and L4, the lamina of L3 and in the head of the 11th rib. Three patients with lesions in close proximity to neural structures (pedicle of T9, the posterolateral inferior aspect of L3 vertebral body and the inferior articular process of C5) were subjected to percutaneous core excision. Mean follow-up was 4.2 +/- 1.6 years. Three out of four patients who underwent radiofrequency ablation had an immediate and sustained response. One patient with a lesion in the head of the rib failed to respond. The three patients in the group of pecutaneous core excisional biopsy demonstrated immediate relief of pain. However, one patient experienced relapse of symptoms 6 months after transpedicular core excision. CT scan suggested partial targeting of the lesion that corroborated with histologic examination revealing only reactive tissue. Subsequent percutaneous core excision was successful. Therefore, the overall success rate was 85.7%. Mean VAS improved dramatically from 9 +/- 1 to 2 +/- 1 after surgery (P < 0.05). No neurological or other complications were encountered. This study indicates that radiofrequency ablation of spinal osteoid osteomas is safe and reasonably effective when an intact cortical shell separates the nidus from the neural elements. Percutaneous core excision can obviate the risk of thermal damage for lesions located in close proximity to the neural elements. Effectiveness of treatment can also be evaluated by CT scan and histological examination. Difficulties in targeting the nidus can lead to treatment failure. The minimal morbidity and the effectiveness of these minimally invasive procedures make them a valid alternative in the treatment of spinal osteoid osteoma.
Figures


References
-
- Aergerter EE, Kirkpatrick JA Jr, editors. Orthopedic diseases. 3. Philadelphia: Saunders; 1968. pp. 491–500.
-
- Assoun J, Railhac JJ, Bonnevialle P, Poey C, Salles de Gauzy J, Baunin C, et al. Osteoid osteoma: percutaneous resection with CT guidance. Radiology. 1993;188(2):541–547. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
