

Cardiovascular magnetic resonance and prognosis in cardiac amyloidosis
- PMID: 19032744
- PMCID: PMC2605441
- DOI: 10.1186/1532-429X-10-54
Cardiovascular magnetic resonance and prognosis in cardiac amyloidosis
Abstract
Background: Cardiac involvement is common in amyloidosis and associated with a variably adverse outcome. We have previously shown that cardiovascular magnetic resonance (CMR) can assess deposition of amyloid protein in the myocardial interstitium. In this study we assessed the prognostic value of late gadolinium enhancement (LGE) and gadolinium kinetics in cardiac amyloidosis in a prospective longitudinal study.
Materials and methods: The pre-defined study end point was all-cause mortality. We prospectively followed a cohort of 29 patients with proven cardiac amyloidosis. All patients underwent biopsy, 2D-echocardiography and Doppler studies, 123I-SAP scintigraphy, serum NT pro BNP assay, and CMR with a T1 mapping method and late gadolinium enhancement (LGE).
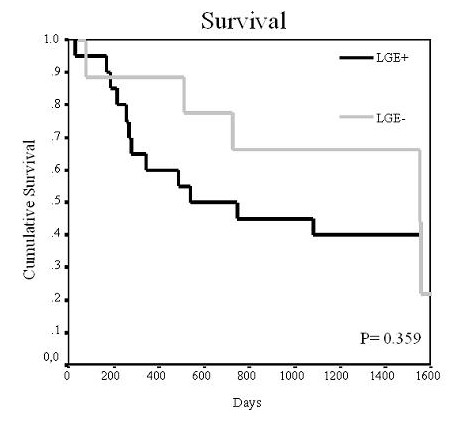
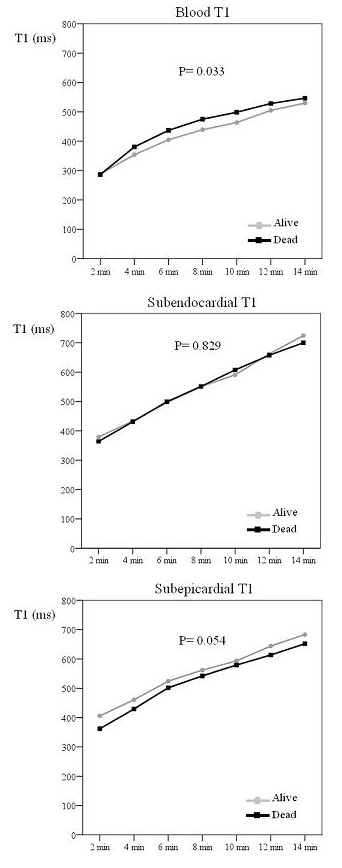
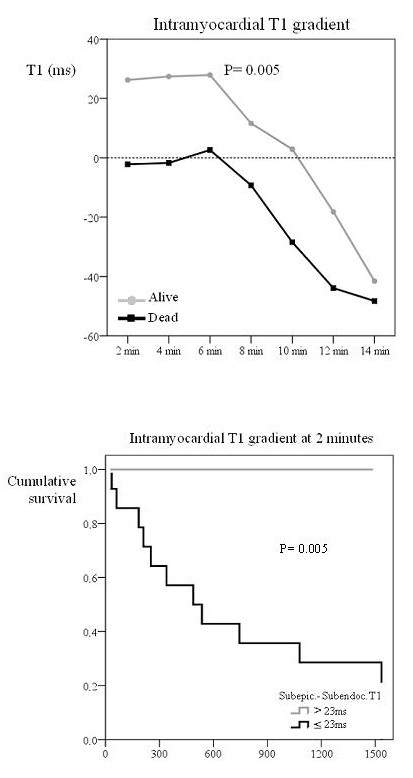
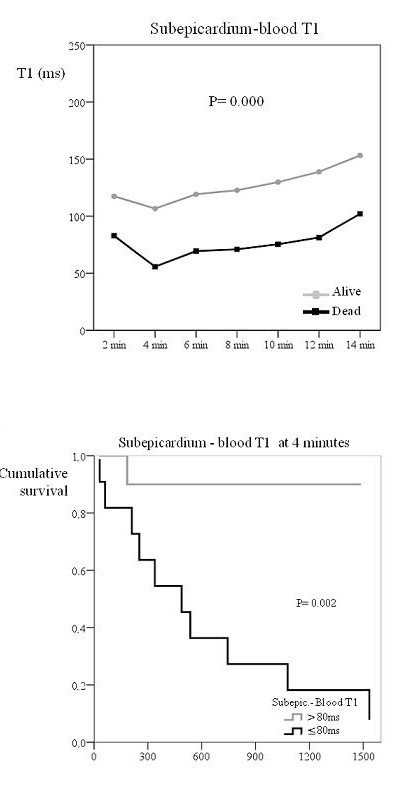
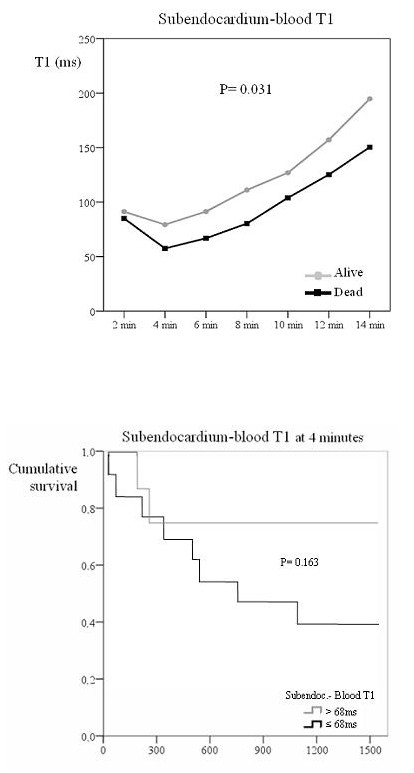
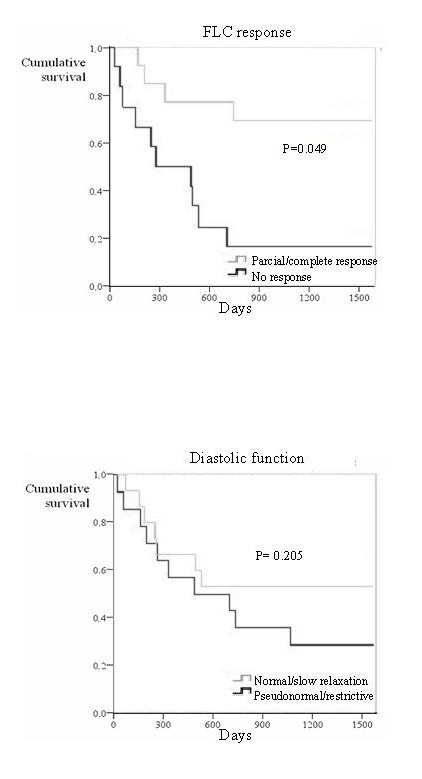
Results: Patients with were followed for a median of 623 days (IQ range 221, 1436), during which 17 (58%) patients died. The presence of myocardial LGE by itself was not a significant predictor of mortality. However, death was predicted by gadolinium kinetics, with the 2 minute post-gadolinium intramyocardial T1 difference between subepicardium and subendocardium predicting mortality with 85% accuracy at a threshold value of 23 ms (the lower the difference the worse the prognosis). Intramyocardial T1 gradient was a better predictor of survival than FLC response to chemotherapy (Kaplan Meier analysis P = 0.049) or diastolic function (Kaplan-Meier analysis P = 0.205).
Conclusion: In cardiac amyloidosis, CMR provides unique information relating to risk of mortality based on gadolinium kinetics which reflects the severity of the cardiac amyloid burden.
Figures
References
-
- Kyle RA, Greipp PR, O'Fallon WM. Primary systemic amyloidosis: multivariate analysis for prognostic factors in 168 cases. Blood. 1986;68:220–4. - PubMed
-
- Arbustini E, Gavazzi A, Merlini G. Fibril-forming proteins: the amyloidosis: new hopes for a disease that cardiologists must know. Ital Heart J Suppl. 2002;3(6):590–597. - PubMed
-
- Nihoyannopoulos P. Amyloid heart disease. Current Opin Cardiol. 1987;2:371–6.
-
- Falk RH, Skinner M. The systemic amyloidoses: an overview. Adv Intern Med. 2000;45:107–137. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
