

Ejection fraction assessment and survival: an analysis of the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT)
- PMID: 19033019
- PMCID: PMC2644051
- DOI: 10.1016/j.ahj.2008.08.007
Ejection fraction assessment and survival: an analysis of the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT)
Abstract
Background: Ejection fraction (EF) is an important method of mortality prediction among cardiac patients, and has been used to identify the highest risk patients for enrollment in the defibrillator primary prevention trials. Evidence suggests that measures of EF by different imaging modalities may not be equivalent. In the SCD-HeFT (Sudden Cardiac Death in Heart Failure Trial), the type of imaging modality for EF assessment was not mandated.
Methods: Baseline assessment of EF was performed using either echocardiography, radionuclide angiography (RNA), or contrast angiography. Multivariable analysis using a Cox proportional hazards model was used to examine whether the modality of assessing EF affected the likelihood of survival.
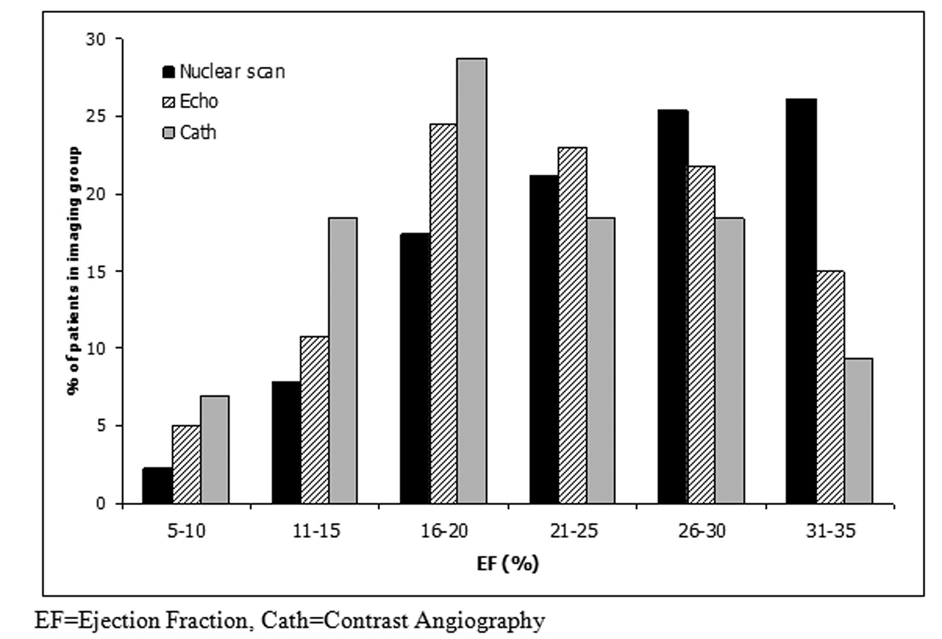
Results: Among the 2,521 patients enrolled in SCD-HeFT, EF was measured by RNA in 616 (24%), echocardiography in 1,469 (58%), and contrast angiography in 436 (17%). Mean EF as measured by RNA was 25.1% +/- 6.9%; by echocardiography, 23.8 +/- 6.9%; and by angiography, 21.9 +/- 6.9%. These measures were significantly different (P < .001), and each pairwise comparison differed significantly (P < .001 for each). Multivariable analysis showed no significant difference in survival between patients enrolled based on RNA versus echocardiography (HR 1.06, 95% CI 0.88-1.28), RNA versus angiography (HR 1.25, 95% CI 0.97-1.62), or echocardiography versus angiography (HR 1.18, 95% CI 0.94-1.48).
Conclusions: Among patients enrolled in SCD-HeFT, the distribution of ejection fractions measured by radionuclide angiography differed from those measured by echocardiography or contrast angiograms. Survival did not differ according to modality of EF assessment.
Figures
References
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N.Engl.J.Med. 2005;352:225–237. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N.Engl.J.Med. 2002;346:877–883. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. Multicenter Automatic Defibrillator Implantation Trial Investigators. N.Engl.J.Med. 1996;335:1933–1940. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N.Engl.J.Med. 1999;341:1882–1890. - PubMed
-
- Hohnloser SH, Kuck KH, Dorian P, et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N.Engl.J.Med. 2004;351:2481–2488. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
